

Late-life factors associated with healthy aging in older men
- PMID: 24779449
- PMCID: PMC4024082
- DOI: 10.1111/jgs.12796
Late-life factors associated with healthy aging in older men
Abstract
Objectives: To identify potentially modifiable late-life biological, lifestyle, and sociodemographic factors associated with overall and healthy survival to age 85.
Design: Prospective longitudinal cohort study with 21 years of follow-up (1991-2012).
Setting: Hawaii Lifespan Study.
Participants: American men of Japanese ancestry (mean age 75.7, range 71-82) without baseline major clinical morbidity and functional impairments (N = 1,292).
Measurements: Overall survival and healthy survival (free from six major chronic diseases and without physical or cognitive impairment) to age 85. Factors were measured at late-life baseline examinations (1991-1993).
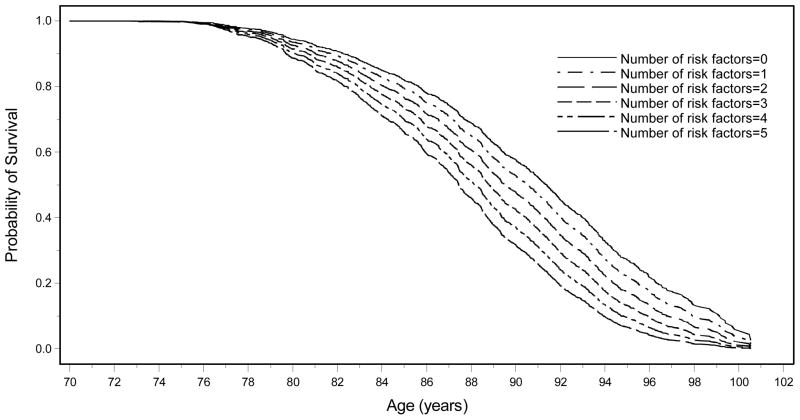
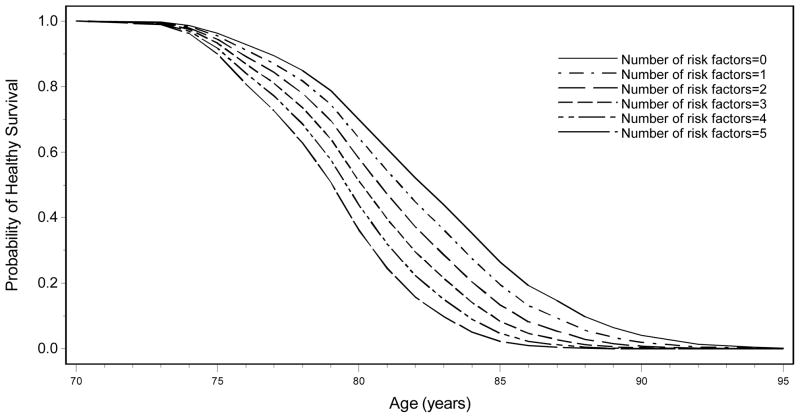
Results: Of 1,292 participants, 1,000 (77%) survived to 85 (34% healthy) and 309 (24%) to 95 (<1% healthy). Late-life factors associated with survival and healthy survival included biological (body mass index, ankle-brachial index, cognitive score, blood pressure, inflammatory markers), lifestyle (smoking, alcohol use, physical activity), and sociodemographic factors (education, marital status). Cumulative late-life baseline risk factor models demonstrated that age-standardized (at 70) probability of survival to 95 ranged from 27% (no factors) to 7% (≥ 5 factors); probability of survival to 100 ranged from 4% (no factors) to 0.1% (≥ 5 factors). Age-standardized (at 70) probability of healthy survival to 90 ranged from 4% (no factors) to 0.01% (≥ 5 factors). There were nine healthy survivors at 95 and one healthy survivor at 100.
Conclusion: Several potentially modifiable risk factors in men in late life (mean age 75.7) were associated with markedly greater probability of subsequent healthy survival and longevity.
Keywords: healthy aging; late-life; longevity; longitudinal cohort study; risk factors.
© 2014, Copyright the Authors Journal compilation © 2014, The American Geriatrics Society.
Conflict of interest statement
Conflict of Interest
Drs. Bell, Masaki, and Curb, Willcox (DCW, BJW) and Poon received grant funding from NIH.
Figures
Similar articles
-
Exceptional longevity in men: modifiable factors associated with survival and function to age 90 years.Arch Intern Med. 2008 Feb 11;168(3):284-90. doi: 10.1001/archinternmed.2007.77. Arch Intern Med. 2008. PMID: 18268169
-
Midlife risk factors and healthy survival in men.JAMA. 2006 Nov 15;296(19):2343-50. doi: 10.1001/jama.296.19.2343. JAMA. 2006. PMID: 17105797
-
150 minutes of vigorous physical activity per week predicts survival and successful ageing: a population-based 11-year longitudinal study of 12 201 older Australian men.Br J Sports Med. 2014 Feb;48(3):220-5. doi: 10.1136/bjsports-2013-092814. Epub 2013 Sep 3. Br J Sports Med. 2014. PMID: 24002240
-
Lifestyle predictors of healthy ageing in men.Maturitas. 2013 Jun;75(2):113-7. doi: 10.1016/j.maturitas.2013.02.011. Epub 2013 Mar 21. Maturitas. 2013. PMID: 23522750 Review.
-
Behavioral determinants of healthy aging.Am J Prev Med. 2005 Apr;28(3):298-304. doi: 10.1016/j.amepre.2004.12.002. Am J Prev Med. 2005. PMID: 15766620 Review.
Cited by
-
Socioeconomic inequalities in frailty and frailty components among community-dwelling older citizens.PLoS One. 2017 Nov 9;12(11):e0187946. doi: 10.1371/journal.pone.0187946. eCollection 2017. PLoS One. 2017. PMID: 29121677 Free PMC article.
-
Ethnic and Gender Disparities in Healthy Ageing among People 50 Years and Older in South Africa.Geriatrics (Basel). 2021 Aug 12;6(3):79. doi: 10.3390/geriatrics6030079. Geriatrics (Basel). 2021. PMID: 34449634 Free PMC article.
-
Annual Review of Asian American Psychology, 2014.Asian Am J Psychol. 2015 Dec;6(4):291-332. doi: 10.1037/aap0000031. Epub 2015 Sep 28. Asian Am J Psychol. 2015. PMID: 26925199 Free PMC article.
-
Survival to Age 90 in Men: The Tromsø Study 1974-2018.Int J Environ Res Public Health. 2019 Jun 6;16(11):2028. doi: 10.3390/ijerph16112028. Int J Environ Res Public Health. 2019. PMID: 31174416 Free PMC article.
-
Physical activity and successful aging among middle-aged and older adults: a systematic review and meta-analysis of cohort studies.Aging (Albany NY). 2020 Apr 29;12(9):7704-7716. doi: 10.18632/aging.103057. Epub 2020 Apr 29. Aging (Albany NY). 2020. PMID: 32350152 Free PMC article.
References
-
- National Institute on Aging. Living Long and Well in the 21st Century - Strategic Directions for Research on Aging. National Institute on Aging. 2007
-
- Olshansky SJ, Perry D, Miller RA, et al. Pursuing the longevity dividend: Scientific goals for an aging world. Ann N Y Acad Sci. 2007;1114:11–13. - PubMed
-
- Fries JF. Aging, natural death, and the compression of morbidity. N Engl J Med. 1980;303:130–135. - PubMed
-
- Curb JD, Guralnik JM, LaCroix AZ, et al. Effective aging. Meeting the challenge of growing older. J Am Geriatr Soc. 1990;38:827–828. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
