

Predicting the occurrence of embolic events: an analysis of 1456 episodes of infective endocarditis from the Italian Study on Endocarditis (SEI)
- PMID: 24779617
- PMCID: PMC4101861
- DOI: 10.1186/1471-2334-14-230
Predicting the occurrence of embolic events: an analysis of 1456 episodes of infective endocarditis from the Italian Study on Endocarditis (SEI)
Abstract
Background: Embolic events are a major cause of morbidity and mortality in patients with infective endocarditis. We analyzed the database of the prospective cohort study SEI in order to identify factors associated with the occurrence of embolic events and to develop a scoring system for the assessment of the risk of embolism.
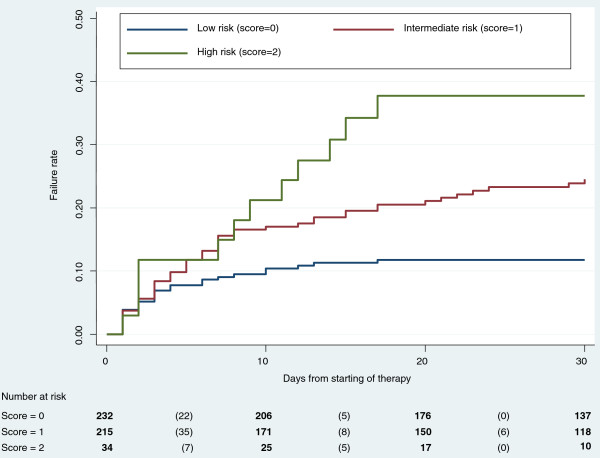
Methods: We retrospectively analyzed 1456 episodes of infective endocarditis from the multicenter study SEI. Predictors of embolism were identified. Risk factors identified at multivariate analysis as predictive of embolism in left-sided endocarditis, were used for the development of a risk score: 1 point was assigned to each risk factor (total risk score range: minimum 0 points; maximum 2 points). Three categories were defined by the score: low (0 points), intermediate (1 point), or high risk (2 points); the probability of embolic events per risk category was calculated for each day on treatment (day 0 through day 30).
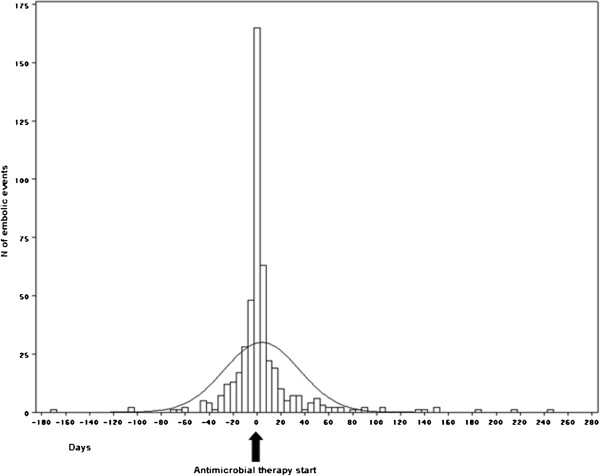
Results: There were 499 episodes of infective endocarditis (34%) that were complicated by ≥ 1 embolic event. Most embolic events occurred early in the clinical course (first week of therapy: 15.5 episodes per 1000 patient days; second week: 3.7 episodes per 1000 patient days). In the total cohort, the factors associated with the occurrence of embolism at multivariate analysis were prosthetic valve localization (odds ratio, 1.84), right-sided endocarditis (odds ratio, 3.93), Staphylococcus aureus etiology (odds ratio, 2.23) and vegetation size ≥ 13 mm (odds ratio, 1.86). In left-sided endocarditis, Staphylococcus aureus etiology (odds ratio, 2.1) and vegetation size ≥ 13 mm (odds ratio, 2.1) were independently associated with embolic events; the 30-day cumulative incidence of embolism varied with risk score category (low risk, 12%; intermediate risk, 25%; high risk, 38%; p < 0.001).
Conclusions: Staphylococcus aureus etiology and vegetation size are associated with an increased risk of embolism. In left-sided endocarditis, a simple scoring system, which combines etiology and vegetation size with time on antimicrobials, might contribute to a better assessment of the risk of embolism, and to a more individualized analysis of indications and contraindications for early surgery.
Figures
References
-
- Thuny F, Avierinos J-F, Tribouilloy C, Giorgi R, Casalta J-P, Milandre L, Brahim A, Nadji G, Riberi A, Collart F, Renard S, Raoult D, Habib G. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur Heart J. 2007;14:1155–1161. doi: 10.1093/eurheartj/ehm005. - DOI - PubMed
-
- Hubert S, Thuny F, Resseguier N, Giorgi R, Tribouilloy C, Le Dolley Y, Casalta J-P, Riberi A, Chevalier F, Rusinaru D, Malaquin D, Remadi JP, Ben Ammar A, Avierinos J-F, Collart F, Raoult D, Habib G. Prediction of symptomatic embolism in infective endocarditis: construction and validation of a risk calculator in a multicenter cohort. J Am Coll Cardiol. 2013;14:1384–1392. doi: 10.1016/j.jacc.2013.07.029. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
