

Detection rate and outcome of colonic serrated epithelial changes in patients with ulcerative colitis or Crohn's colitis
- PMID: 24779703
- PMCID: PMC4894660
- DOI: 10.1111/apt.12774
Detection rate and outcome of colonic serrated epithelial changes in patients with ulcerative colitis or Crohn's colitis
Abstract
Background: Chronic ulcerative colitis (CUC) and colonic Crohn's disease (CD) increase colorectal neoplasia (CRN) risk. While sessile serrated polyp (SSP) is a known cancer precursor, serrated epithelial changes (SEC) are of uncertain prevalence and neoplastic risk.
Aim: To assess the serrated lesion detection rates in CUC and CD and documented incidence of subsequent CRN in a retrospective, single-centre cohort study.
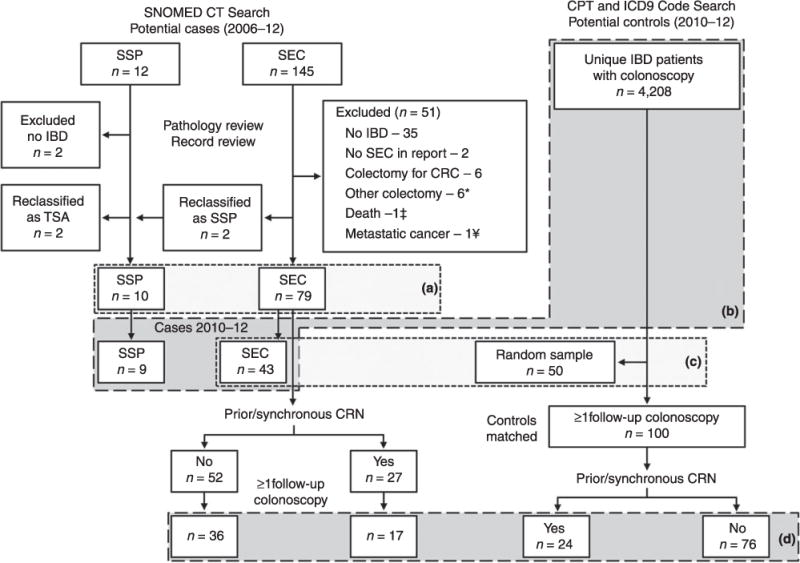
Methods: Patients were identified by a central diagnostic index and pathology review confirmed SEC, SSP, CUC and CD diagnoses from 2006-12. Matched controls were identified from among all CUC and CD patients having colonoscopy during the second half of the time period. All were followed for incident CRN, estimated by the Kaplan-Meier method.
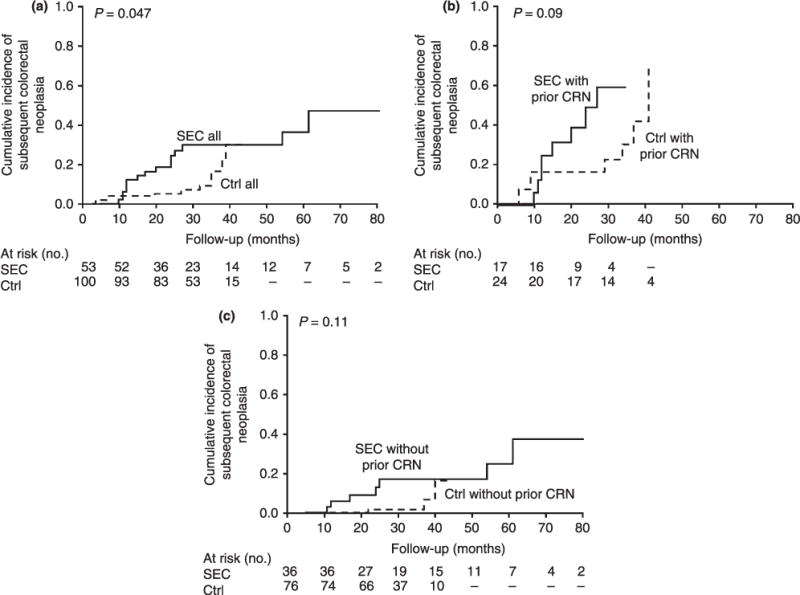
Results: Between 2006 and 2012, 79 SEC and 10 SSP cases were identified. Detection rates were estimated to be 10/1000 and 2/1000 patients, for SEC and SSP respectively, among 4208 unique CUC or CD patients having colonoscopy from 2010-12. With only 10 cases, SSP patients were not further analysed. Cumulative incidence of subsequent CRN at 1 and 3 years was 12% (95% CI, 0-30%) and 30% (3-57%), respectively, in SEC patients compared to 4% (0-12%) and 9% (0-23%), respectively, in CUC or CD controls (P = 0.047, log-rank). However, this statistical difference was not significant after patients were stratified for history of prior or synchronous dysplasia (P = 0.09).
Conclusions: Serrated epithelial changes and sessile serrated polyps are uncommonly detected by colonoscopy in chronic ulcerative colitis and Crohn's disease patients. Histology with changes of serrated epithelium may be associated with risk of subsequent colorectal neoplasia, however further studies are needed to explore this relationship.
© 2014 John Wiley & Sons Ltd.
Figures
References
-
- Munkholm P. Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease. Aliment Pharmacol Ther. 2003;18(Suppl 2):1–5. - PubMed
-
- Jess T, Rungoe C, Peyrin-Biroulet L. Risk of colorectal cancer in patients with ulcerative colitis: a meta-analysis of population-based cohort studies. Clin Gastroenterol Hepatol. 2012;10:639–45. - PubMed
-
- Herrinton LJ, Liu L, Levin TR, Allison JE, Lewis JD, Velayos F. Incidence and mortality of colorectal adenocarcinoma in persons with inflammatory bowel disease from 1998 to 2010. Gastroenterology. 2012;143:382–9. - PubMed
-
- Farmer RG, Hawk WA, Turnbull RB., Jr Carcinoma associated with mucosal ulcerative colitis, and with transmural colitis and enteritis (Crohn’s disease) Cancer. 1971;28:289–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous