

A single surgeon's series of transthoracic oesophageal resections
- PMID: 24780676
- PMCID: PMC4474246
- DOI: 10.1308/003588414X13814021677359
A single surgeon's series of transthoracic oesophageal resections
Abstract
Introduction: Significant controversy persists over the optimum surgical management of oesophageal carcinoma. The authors report on a consecutive personal series of open transthoracic oesophageal resections.
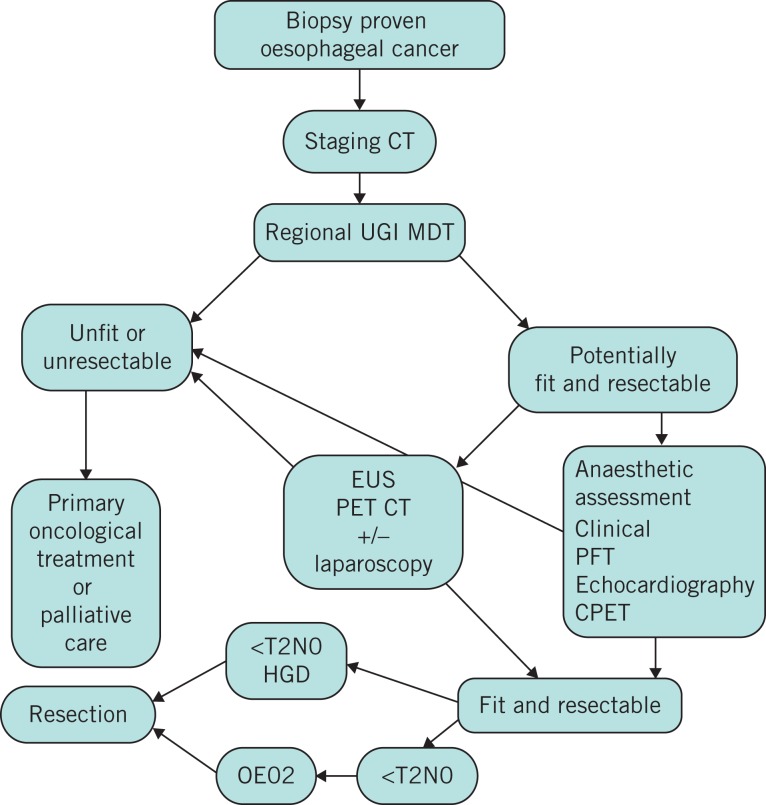
Methods: Data relating to resections performed between mid-1993 and the end of 2010 were analysed. Patient and tumour assessment evolved over this period. Preoperative chemotherapy in appropriate cases was introduced in 2002. A laparotomy and right lateral thoracotomy approach (Ivor-Lewis) was used. In all cases the pylorus was not interfered with, no attempt was made to perform a radical lymphadenectomy but surgical strategy was focused on producing an R0 resection and a hand sewn anastomosis was fashioned.
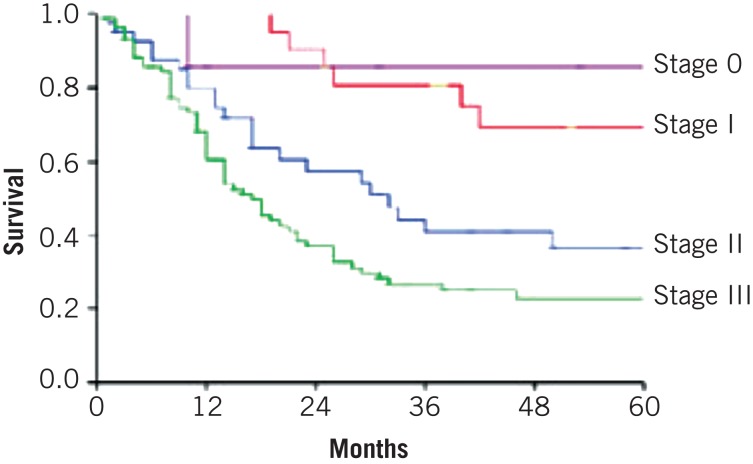
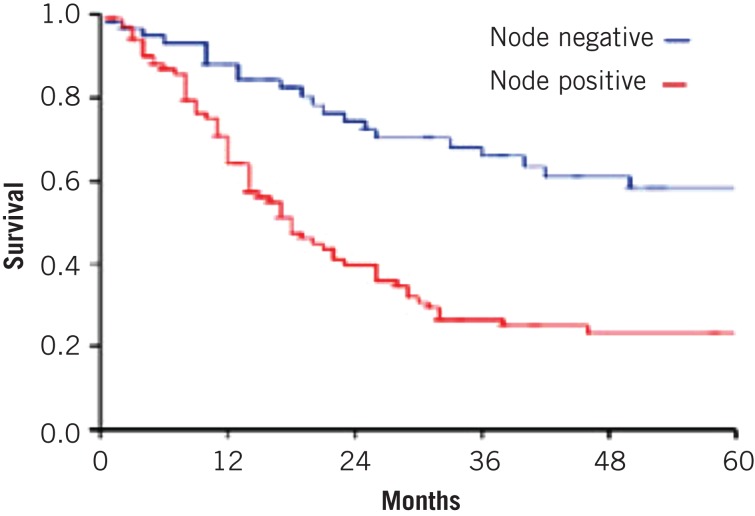
Results: A total of 165 resections were performed; 130 patients (80%) were male. The median age was 66 years (range: 31-82 years). Eighty per cent had an adenocarcinoma. Sixty-four per cent of the tumours were T3/T4 and sixty-two per cent node positive. Forty patients (24%) had an involved circumferential resection margin (CRM). Five patients (3.0%) had no resection and a quarter (26%) developed morbidity of some form. There was one clinical anastomotic leak (0.6%) and three benign strictures requiring dilation (1.8%). In-hospital mortality was 3.0% (5 patients). Disease specific survival at one, two and five years was 77%, 42% and 36% respectively. Neither CRM involvement nor preoperative chemotherapy influenced survival significantly. No patient required intervention to disrupt the pylorus.
Conclusions: Excellent outcomes are achievable following open transthoracic oesophagectomy without radical lymphadenectomy using a hand sewn gastro-oesophageal anastomosis and without disrupting the pylorus.
Figures
References
-
- Oesophageal Cancer Key Facts Cancer Research UK. http://www.cancerresearchuk.org/cancer-info/cancerstats/keyfacts/oesopha... (cited November 2013).
-
- Muller JM, Erasmi H, Stelzner M, et al. Surgical therapy of oesophageal carcinoma. Br J Surg. 1990;77:845–57. - PubMed
-
- Sanghera SS, Nurkin SJ, Demmy TL. Quality of life after an esophagectomy. Surg Clin North Am. 2012;92:1,315–1,335. - PubMed
-
- Heath EI, Kaufman HS, Talamini MA, et al. The role of laparoscopy in preoperative staging of esophageal cancer. Surg Endosc. 2000;14:495–499. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical