

Progressive hearing loss and vestibular dysfunction caused by a homozygous nonsense mutation in CLIC5
- PMID: 24781754
- PMCID: PMC4297911
- DOI: 10.1038/ejhg.2014.83
Progressive hearing loss and vestibular dysfunction caused by a homozygous nonsense mutation in CLIC5
Abstract
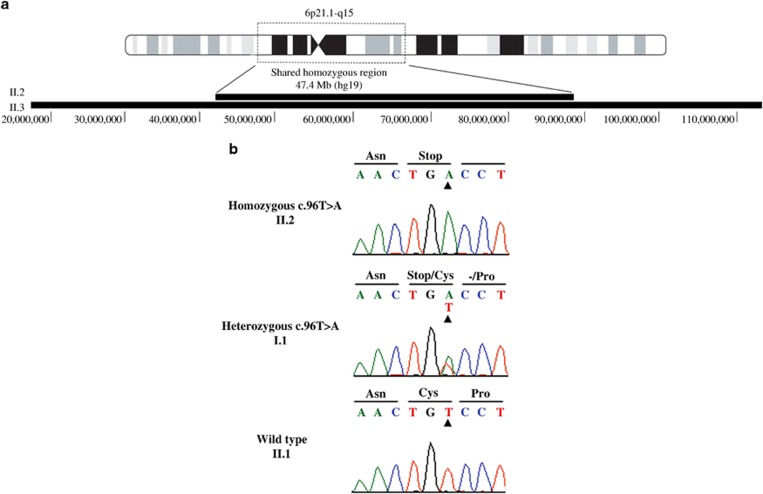
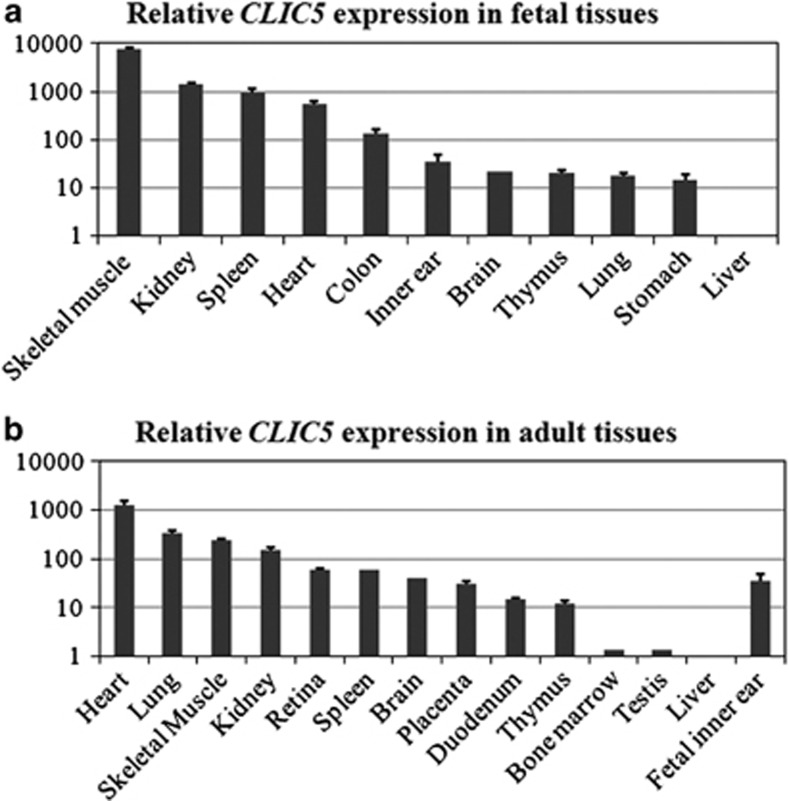
In a consanguineous Turkish family diagnosed with autosomal recessive nonsyndromic hearing impairment (arNSHI), a homozygous region of 47.4 Mb was shared by the two affected siblings on chromosome 6p21.1-q15. This region contains 247 genes including the known deafness gene MYO6. No pathogenic variants were found in MYO6, neither with sequence analysis of the coding region and splice sites nor with mRNA analysis. Subsequent candidate gene evaluation revealed CLIC5 as an excellent candidate gene. The orthologous mouse gene is mutated in the jitterbug mutant that exhibits progressive hearing impairment and vestibular dysfunction. Mutation analysis of CLIC5 revealed a homozygous nonsense mutation c.96T>A (p.(Cys32Ter)) that segregated with the hearing loss. Further analysis of CLIC5 in 213 arNSHI patients from mostly Dutch and Spanish origin did not reveal any additional pathogenic variants. CLIC5 mutations are thus not a common cause of arNSHI in these populations. The hearing loss in the present family had an onset in early childhood and progressed from mild to severe or even profound before the second decade. Impaired hearing is accompanied by vestibular areflexia and in one of the patients with mild renal dysfunction. Although we demonstrate that CLIC5 is expressed in many other human tissues, no additional symptoms were observed in these patients. In conclusion, our results show that CLIC5 is a novel arNSHI gene involved in progressive hearing impairment, vestibular and possibly mild renal dysfunction in a family of Turkish origin.
Figures

References
-
- Mehl AL, Thomson V. The Colorado newborn hearing screening project, 1992-1999: on the threshold of effective population-based universal newborn hearing screening. Pediatrics. 2002;109:E7. - PubMed
-
- Dror AA, Avraham KB. Hearing loss: mechanisms revealed by genetics and cell biology. Annu Rev Genet. 2009;43:411–437. - PubMed
-
- Delmaghani S, Aghaie A, Michalski N, Bonnet C, Weil D, Petit C. Defect in the gene encoding the EAR/EPTP domain-containing protein TSPEAR causes DFNB98 profound deafness. Hum Mol Genet. 2012;21:3835–3844. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
