

Long-term safety of subcutaneous abatacept in rheumatoid arthritis: integrated analysis of clinical trial data representing more than four years of treatment
- PMID: 24782324
- PMCID: PMC4309516
- DOI: 10.1002/art.38687
Long-term safety of subcutaneous abatacept in rheumatoid arthritis: integrated analysis of clinical trial data representing more than four years of treatment
Abstract
Objective: To investigate the safety of long-term subcutaneous (SC) abatacept treatment using integrated clinical trial data obtained in patients with rheumatoid arthritis refractory to traditional disease-modifying antirheumatic drugs.
Methods: Data from the double-blind and open-label phases of 5 clinical trials of SC abatacept were pooled. The overall and 6-month incidence rates were calculated as events per 100 patient-years of exposure.
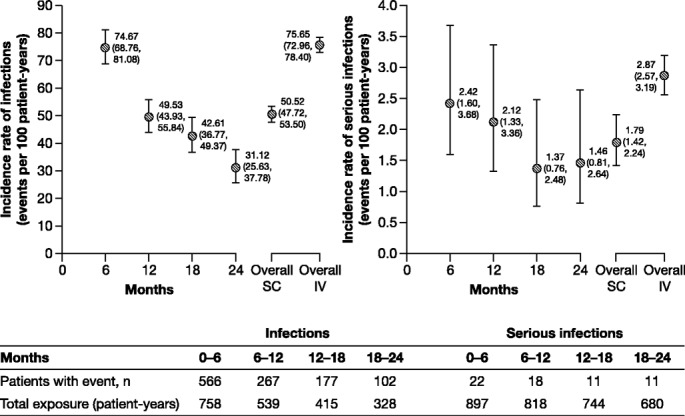
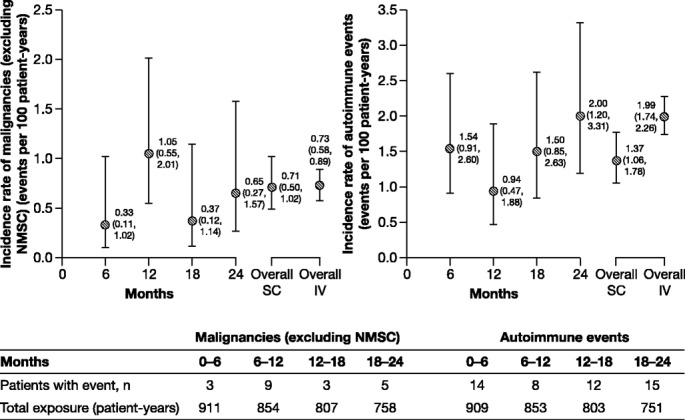
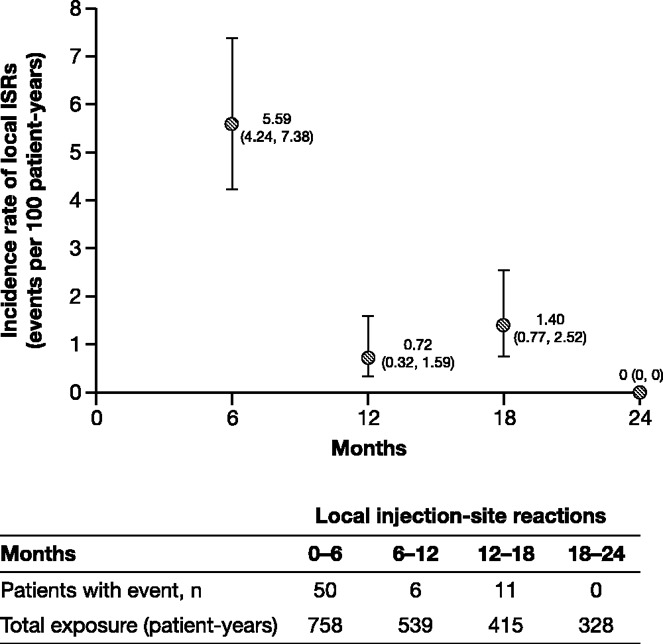
Results: This analysis included 1,879 patients with 4,214.6 patient-years of exposure to SC abatacept. The mean ± SD length of exposure was 27.3 ± 9.1 months. The reported incidence rate of serious infections was 1.79 (95% confidence interval [95% CI] 1.42-2.24); the most frequent infections were pneumonia (incidence rate 0.36 [95% CI 0.22-0.59]), urinary tract infection (incidence rate 0.14 [95% CI 0.06-0.32]), and gastroenteritis (incidence rate 0.10 [95% CI 0.04-0.25]). Tuberculosis occurred rarely (incidence rate 0.09 [95% CI 0.04-0.25]). The reported incidence rate of malignancies was 1.32 (95% CI 1.01-1.72), and the most common was solid organ malignancy (incidence rate 0.69 [95% CI 0.48-0.99]). The incidence rate of autoimmune events was 1.37 (95% CI 1.06-1.78), and the most frequent events were psoriasis (incidence rate 0.33 [95% CI 0.20-0.56]) and Sjögren's syndrome (incidence rate 0.24 [95% CI 0.13-0.44]). The reported incidence rate of local injection site reactions was 1.72 (95% CI 1.36-2.17); these events occurred primarily during the first 6 months of treatment, and almost all were of mild or moderate intensity. The incidence rates of serious infections, malignancies, autoimmune events, and injection site reactions did not increase over time.
Conclusion: Long-term treatment with SC abatacept was associated with low incidence rates of serious infections, malignancies, and autoimmune events and was well tolerated, with infrequent injection site reactions. These findings are consistent with those related to treatment with intravenous abatacept. Long-term treatment with SC abatacept did not lead to new safety signals over time.
Copyright © 2014 by the American College of Rheumatology.
Figures
References
-
- Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Allaart CF, van Zeben D, Kerstens PJ, Hazes JM. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): a randomized, controlled trial. Arthritis Rheum. 2005;52:3381–90. , et al. - PubMed
-
- Dore RK, Mathews S, Schechtman J, Surbeck W, Mandel D, Patel A. The immunogenicity, safety, and efficacy of etanercept liquid administered once weekly in patients with rheumatoid arthritis. Clin Exp Rheumatol. 2007;25:40–6. , et al. - PubMed
-
- Bartelds GM, Krieckaert CL, Nurmohamed MT, van Schouwenburg PA, Lems WF, Twisk JW. Development of antidrug antibodies against adalimumab and association with disease activity and treatment failure during long-term follow-up. JAMA. 2011;305:1460–8. , et al. - PubMed
-
- Radstake TR, Svenson M, Eijsbouts AM, van den Hoogen FH, Enevold C, van Riel PL. Formation of antibodies against infliximab and adalimumab strongly correlates with functional drug levels and clinical responses in rheumatoid arthritis. Ann Rheum Dis. 2009;68:1739–45. , et al. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
