

Thyroid function and obesity
- PMID: 24783015
- PMCID: PMC3821486
- DOI: 10.1159/000342994
Thyroid function and obesity
Abstract
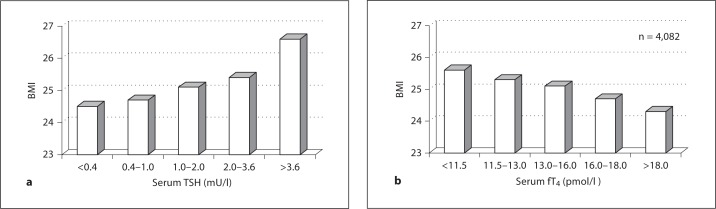
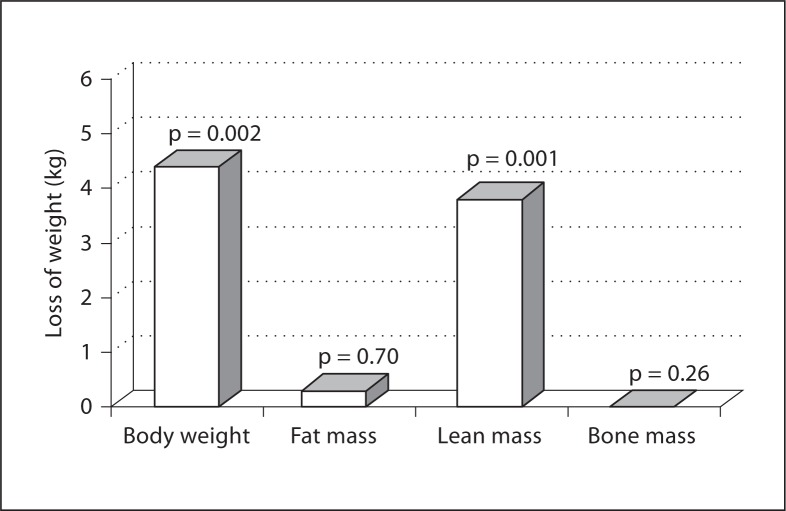
Important interaction exists between thyroid function, weight control, and obesity. Several mechanisms seem to be involved, and in studies of groups of people the pattern of thyroid function tests depends on the balance of obesity and underlying thyroid disease in the cohort studied. Obese people with a normal thyroid gland tend to have activation of the hypothalamic-pituitary-thyroid axis with higher serum TSH and thyroid hormones in serum. On the other hand, small differences in thyroid function are associated with up to 5 kg difference in body weight. The weight loss after therapy of overt hypothyroidism is caused by excretion of water bound in tissues (myxoedema). Many patients treated for hyperthyroidism experience a gain of more weight than they lost during the active phase of the disease. The mechanism for this excessive weight gain has not been fully elucidated. New studies on the relation between L-T3 therapy and weight control are discussed. The interaction between weight control and therapy of thyroid disease is important to many patients and it should be studied in more detail.
Keywords: Graves’ disease; Hyperthyroidism; Hypothyroidism; Levothyroxine therapy; Liothyronine therapy; Obesity; Thyroid function; Weight control.
Figures

References
-
- Caballero B. The global epidemic of obesity: an overview. Epidemiol Rev. 2007;29:1–5. - PubMed
-
- Aeberli I, Ammann RS, Knabenhans M, Molinari L, Zimmermann MB. Decrease in the prevalence of paediatric adiposity in Switzerland from 2002 to 2007. Public Health Nutr. 2010;13:806–811. - PubMed
-
- Svendstrup M, Knudsen NK, Jørgensen T, Rasmussen LB, Ovesen L, Perrild H, Laurberg P. Stagnation in body mass index in Denmark from 1997/1998 to 2004/2005, but with geographical diversity. Dan Med Bul. 2011;58:1–5. - PubMed
-
- Rinaldi S, Lise M, Clavel-Chapelon F, Boutron-Ruault MC, Guillas G, Overvad K, Tjønneland A, Halkjaer J, Lukanova A, Kaaks R, Bergmann MM, Boeing H, Trichopoulou A, Zylis D, Valanou E, Palli D, Agnoli C, Tumino R, Polidoro S, Mattiello A, Bas Bueno-de-Mesquita H, Peeters PH, Weiderpass E, Lund E, Skeie G, Rodríguez L, Travier N, Sánchez MJ, Amiano P, Huerta JM, Ardanaz E, Rasmuson T, Hallmans G, Almquist M, Manjer J, Tsilidis KK, Allen NE, Khaw KT, Wareham N, Byrnes G, Romieu I, Riboli E, Franceschi S. Body size and risk of differentiated thyroid carcinomas: findings from the EPIC study. Int J Cancer. 2012;131:E1004–E1014. - PubMed
-
- Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008;371:569–578. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
