

Standardized Ultrasound Report for Thyroid Nodules: The Endocrinologist's Viewpoint
- PMID: 24783037
- PMCID: PMC3821499
- DOI: 10.1159/000347144
Standardized Ultrasound Report for Thyroid Nodules: The Endocrinologist's Viewpoint
Abstract
Background: Ultrasonography (US) plays a crucial role in the diagnostic management of thyroid nodules, but its widespread use in clinical practice might generate heterogeneity in ultrasound reports.
Objectives: The aims of the study were to propose (a) a standardized lexicon for description of thyroid nodules in order to reduce US reports of interobserver variability and (b) a US classification system of suspicion for thyroid nodules in order to promote a uniform management of thyroid nodules.
Methods: RELEVANT PUBLISHED ARTICLES WERE IDENTIFIED BY SEARCHING MEDLINE AT PUBMED COMBINING THE FOLLOWING SEARCH TERMS: ultrasonography, thyroid, nodule, malignancy, carcinoma, and classification system. Results were supplemented with our data and experience.
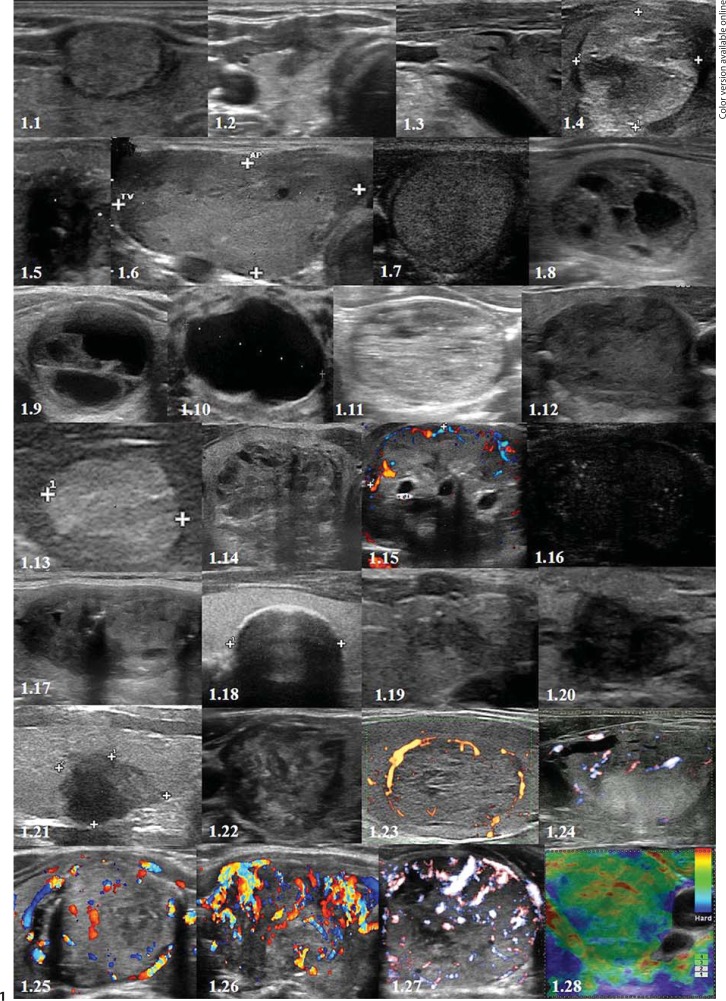
Results: A STANDARDIZED US REPORT SHOULD ALWAYS DOCUMENT POSITION, EXTRACAPSULAR RELATIONSHIPS, NUMBER, AND THE FOLLOWING CHARACTERISTICS OF EACH THYROID LESION: shape, internal content, echogenicity, echotexture, presence of calcifications, margins, vascularity, and size. Combining the previous US features, each thyroid nodule can be tentatively classified as: malignant, suspicious for malignancy, borderline, probably benign, and benign.
Conclusions: We propose a standardized US report and a tentative US classification system that may become helpful for endocrinologists dealing with thyroid nodules in their clinical practice. The proposed classification does not allow to bypass the required cytological confirmation, but may become useful in identifying the lesions with a lower risk of neoplasm.
Keywords: Carcinoma; Elastography; Malignancy; Nodule; Thyroid; Tumor; Ultrasonography; Ultrasound.
Figures
References
-
- Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med. 1993;328:553–559. - PubMed
-
- Ezzat S, Sarti DA, Cain DR, Braunstein GD. Thyroid incidentalomas. Prevalence by palpation and ultrasonography. Arch Intern Med. 1994;154:1838–1840. - PubMed
-
- Gharib H, Papini E, Valcavi R, Baskin HJ, Crescenzi A, Dottorini ME, Duick DS, Guglielmi R, Hamilton CR, Jr, Zeiger MA, Zini M. AACE/AME Task Force on Thyroid Nodules. American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract. 2006;12:63–102. - PubMed
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006;295:2164–2167. - PubMed
-
- Gharib H. Fine-needle aspiration biopsy of the thyroid nodules: advantages, limitations and effect. Mayo Clinic Proc. 1994;69:44–49. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
