

2013 ETA Guideline: Management of Subclinical Hypothyroidism
- PMID: 24783053
- PMCID: PMC3923601
- DOI: 10.1159/000356507
2013 ETA Guideline: Management of Subclinical Hypothyroidism
Abstract
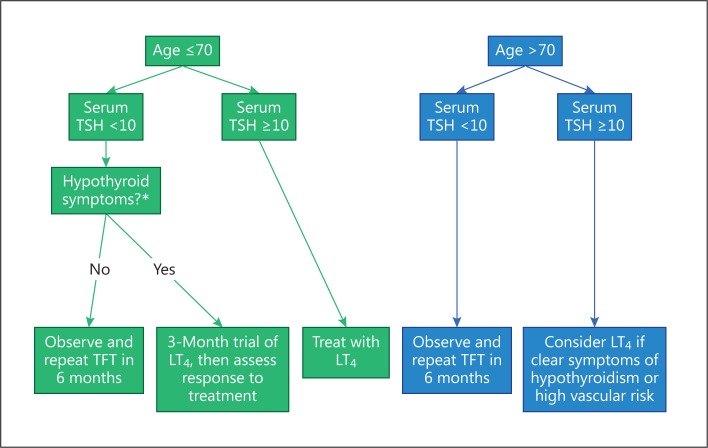
Subclinical hypothyroidism (SCH) should be considered in two categories according to the elevation in serum thyroid-stimulating hormone (TSH) level: mildly increased TSH levels (4.0-10.0 mU/l) and more severely increased TSH value (>10 mU/l). An initially raised serum TSH, with FT4 within reference range, should be investigated with a repeat measurement of both serum TSH and FT4, along with thyroid peroxidase antibodies, preferably after a 2- to 3-month interval. Even in the absence of symptoms, replacement therapy with L-thyroxine is recommended for younger patients (<65-70 years) with serum TSH >10 mU/l. In younger SCH patients (serum TSH <10 mU/l) with symptoms suggestive of hypothyroidism, a trial of L-thyroxine replacement therapy should be considered. For such patients who have been started on L-thyroxine for symptoms attributed to SCH, response to treatment should be reviewed 3 or 4 months after a serum TSH within reference range is reached. If there is no improvement in symptoms, L-thyroxine therapy should generally be stopped. Age-specific local reference ranges for serum TSH should be considered in order to establish a diagnosis of SCH in older people. The oldest old subjects (>80-85 years) with elevated serum TSH ≤10 mU/l should be carefully followed with a wait-and-see strategy, generally avoiding hormonal treatment. If the decision is to treat SCH, then oral L-thyroxine, administered daily, is the treatment of choice. The serum TSH should be re-checked 2 months after starting L-thyroxine therapy, and dosage adjustments made accordingly. The aim for most adults should be to reach a stable serum TSH in the lower half of the reference range (0.4-2.5 mU/l). Once patients with SCH are commenced on L-thyroxine treatment, then serum TSH should be monitored at least annually thereafter.
Keywords: Cognition; L-Thyroxine; Management; Subclinical hypothyroidism; Thyrotropin; Vascular risk.
Figures
References
-
- Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The Colorado thyroid disease prevalence study. Arch Intern Med. 2000;160:526–534. - PubMed
-
- Vanderpump MP, Tunbridge WM, French JM, et al. The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol. 1995;43:55–68. - PubMed
-
- Surks MI, Ortiz E, Daniels GH, et al. Subclinical thyroid disease: scientific review and guidelines for diagnosis and management. JAMA. 2004;29:228–238. - PubMed
-
- Kunz R, Vigersky RA, Guyatt GH, Montori VM. A case for clarity, consistency, and helpfulness: state-of-the-art clinical practice guidelines in endocrinology using the grading of recommendations, assessment, development, and evaluation system. J Clin Endocrinol Metab. 2008;93:666–673. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
