

Optimal management of the critically ill: anaesthesia, monitoring, data capture, and point-of-care technological practices in ovine models of critical care
- PMID: 24783206
- PMCID: PMC3982457
- DOI: 10.1155/2014/468309
Optimal management of the critically ill: anaesthesia, monitoring, data capture, and point-of-care technological practices in ovine models of critical care
Abstract
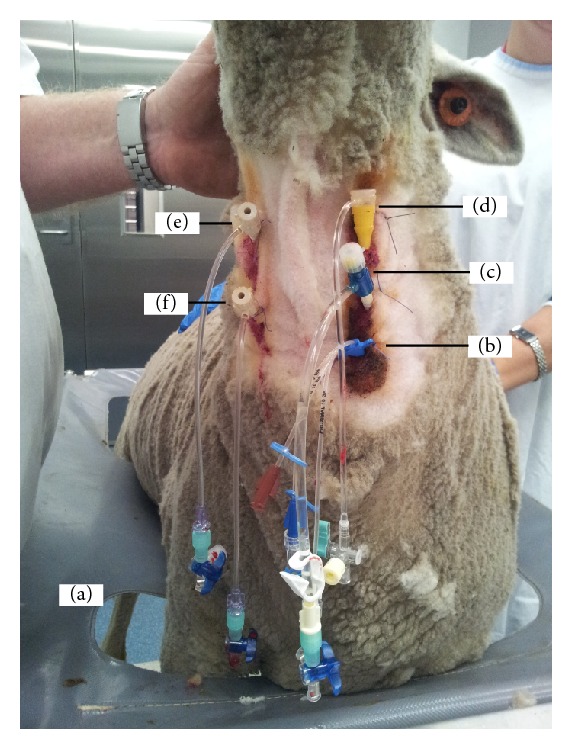
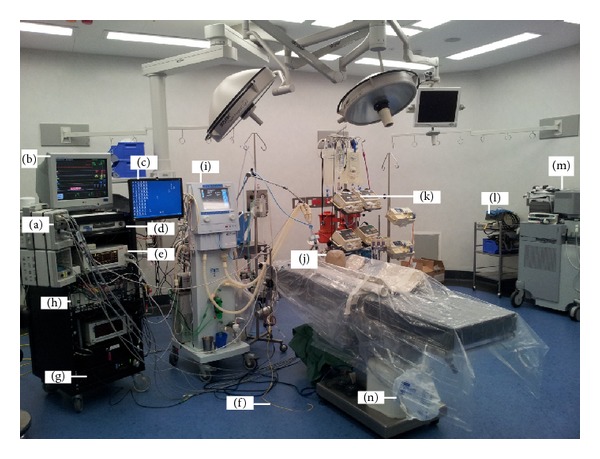
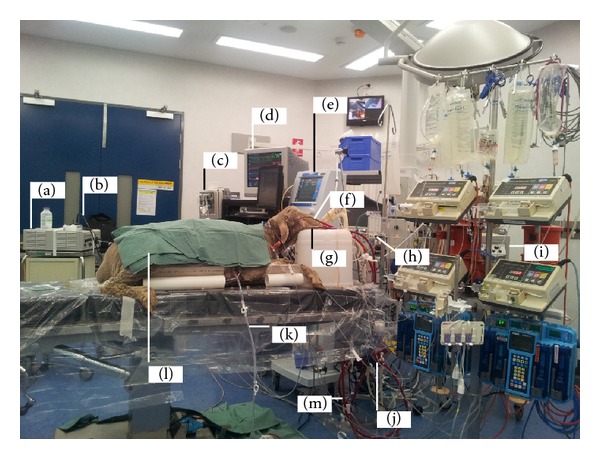
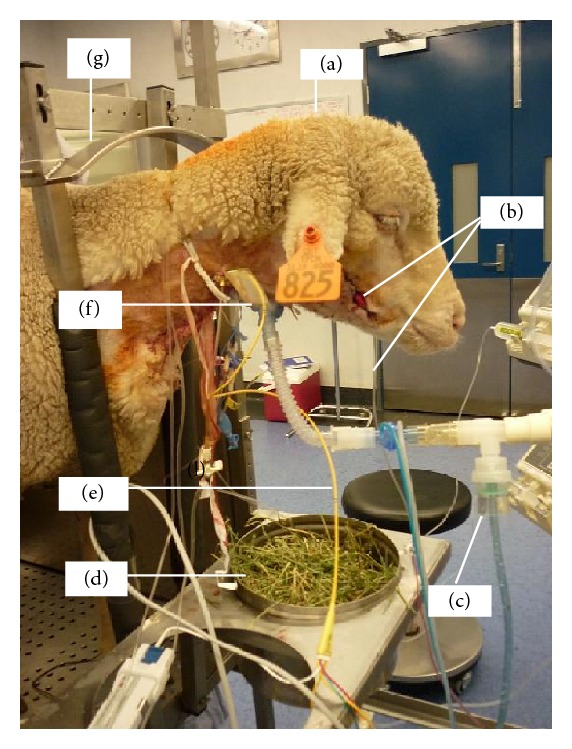
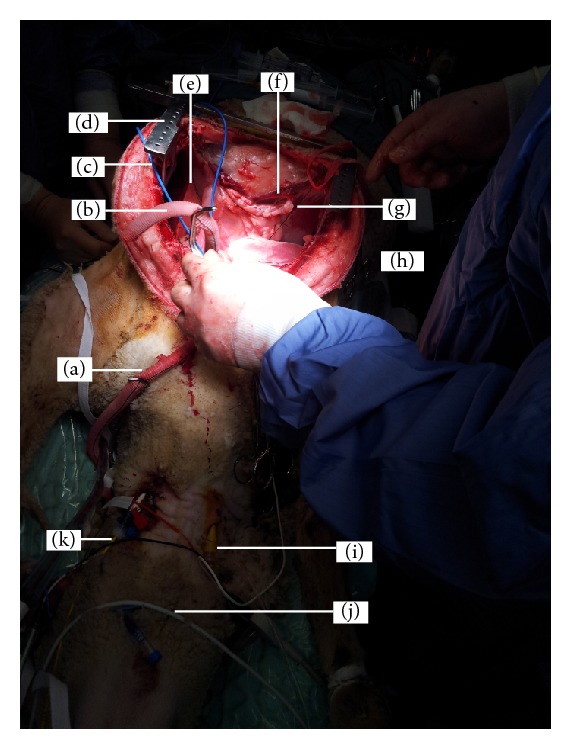
Animal models of critical illness are vital in biomedical research. They provide possibilities for the investigation of pathophysiological processes that may not otherwise be possible in humans. In order to be clinically applicable, the model should simulate the critical care situation realistically, including anaesthesia, monitoring, sampling, utilising appropriate personnel skill mix, and therapeutic interventions. There are limited data documenting the constitution of ideal technologically advanced large animal critical care practices and all the processes of the animal model. In this paper, we describe the procedure of animal preparation, anaesthesia induction and maintenance, physiologic monitoring, data capture, point-of-care technology, and animal aftercare that has been successfully used to study several novel ovine models of critical illness. The relevant investigations are on respiratory failure due to smoke inhalation, transfusion related acute lung injury, endotoxin-induced proteogenomic alterations, haemorrhagic shock, septic shock, brain death, cerebral microcirculation, and artificial heart studies. We have demonstrated the functionality of monitoring practices during anaesthesia required to provide a platform for undertaking systematic investigations in complex ovine models of critical illness.
Figures
References
-
- Traber DL, Maybauer MO, Maybauer DM, Westphal M, Traber LD. Inhalational and acute lung injury. Shock. 2005;24(supplement 1):82–87. - PubMed
-
- Shekar K, Fung YL, Diab S, et al. Development of simulated and ovine models of extracorporeal life support to improve understanding of circuit-host interactions. Critical Care and Resuscitation. 2012;14(2):105–111. - PubMed
-
- Hein WR, Griebel PJ. A road less travelled: large animal models in immunological research. Nature Reviews Immunology. 2003;3(1):79–84. - PubMed
-
- Walters EM, Agca Y, Ganjam V, Evans T. Animal models got you puzzled?: think pig. Annals of the New York Academy of Sciences. 2011;1245(1):63–64. - PubMed
-
- Nunoya T, Shibuya K, Saitoh T, et al. Use of miniature pig for biomedical research, with reference to toxicologic studies. Journal of Toxicologic Pathology. 2007;20(3):125–132.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
