

Effect of a genomic classifier test on clinical practice decisions for patients with high-risk prostate cancer after surgery
- PMID: 24784420
- PMCID: PMC4371645
- DOI: 10.1111/bju.12789
Effect of a genomic classifier test on clinical practice decisions for patients with high-risk prostate cancer after surgery
Abstract
Objectives: To evaluate the impact of a genomic classifier (GC) test for predicting metastasis risk after radical prostatectomy (RP) on urologists' decision-making about adjuvant treatment of patients with high-risk prostate cancer.
Subjects and methods: Patient case history was extracted from the medical records of each of the 145 patients with pT3 disease or positive surgical margins (PSMs) after RP treated by six high-volume urologists, from five community practices. GC results were available for 122 (84%) of these patients. US board-certified urologists (n = 107) were invited to provide adjuvant treatment recommendations for 10 cases randomly drawn from the pool of patient case histories. For each case, the study participants were asked to make an adjuvant therapy recommendation without (clinical variables only) and with knowledge of the GC test results. Recommendations were made without knowledge of other participants' responses and the presentation of case histories was randomised to minimise recall bias.
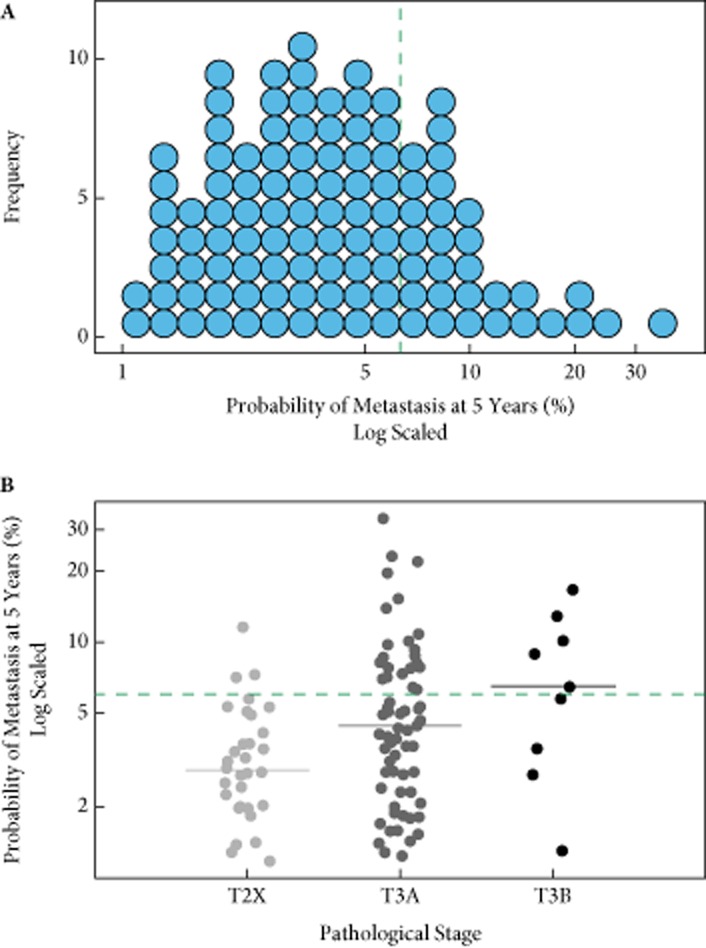
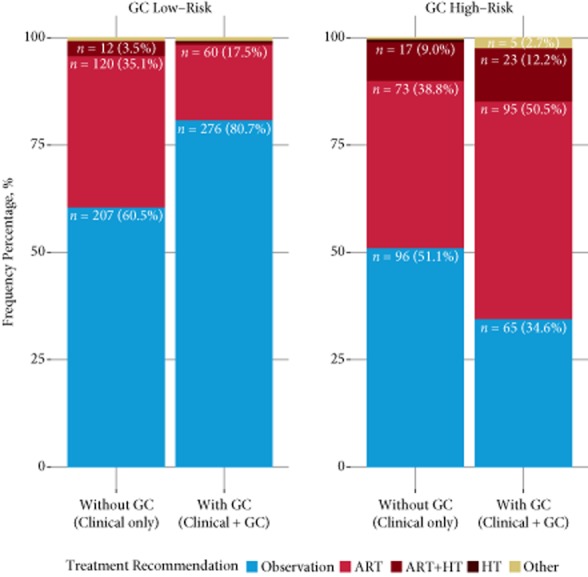
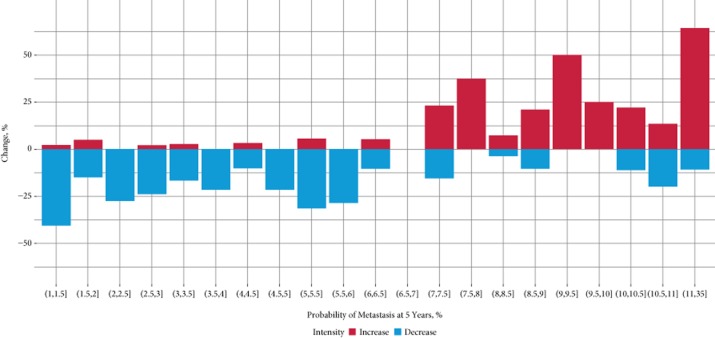
Results: A total of 110 patient case histories were available for review by the study participants. The median patient age was 62 years, 71% of patients had pT3 disease and 63% had PSMs. The median (range) 5-year predicted probability of metastasis by the GC test for the cohort was 3.9 (1-33)% and the GC test classified 72% of patients as having low risk for metastasis. A total of 51 urologists consented to the study and provided 530 adjuvant treatment recommendations without, and 530 with knowledge of the GC test results. Study participants performed a mean of 130 RPs/year and 55% were from community-based practices. Without GC test result knowledge, observation was recommended for 57% (n = 303), adjuvant radiation therapy (ART) for 36% (n = 193) and other treatments for 7% (n = 34) of patients. Overall, 31% (95% CI: 27-35%) of treatment recommendations changed with knowledge of the GC test results. Of the ART recommendations without GC test result knowledge, 40% (n = 77) changed to observation (95% CI: 33-47%) with this knowledge. Of patients recommended for observation, 13% (n = 38 [95% CI: 9-17%]) were changed to ART with knowledge of the GC test result. Patients with low risk disease according to the GC test were recommended for observation 81% of the time (n = 276), while of those with high risk, 65% were recommended for treatment (n = 118; P < 0.001). Treatment intensity was strongly correlated with the GC-predicted probability of metastasis (P < 0.001) and the GC test was the dominant risk factor driving decisions in multivariable analysis (odds ratio 8.6, 95% CI: 5.3-14.3%; P < 0.001).
Conclusions: Knowledge of GC test results had a direct effect on treatment strategies after surgery. Recommendations for observation increased by 20% for patients assessed by the GC test to be at low risk of metastasis, whereas recommendations for treatment increased by 16% for patients at high risk of metastasis. These results suggest that the implementation of genomic testing in clinical practice may lead to significant changes in adjuvant therapy decision-making for high-risk prostate cancer.
Keywords: clinical practice; decision impact; metastasis; patient management; prognosis; prostate cancer.
© 2014 The Authors. BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Figures

References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer Statistics, 2014. CA Cancer J Clin. 2014;64:9–29. - PubMed
-
- Swanson GP, Riggs M, Hermans M. Pathologic findings at radical prostatectomy: risk factors for failure and death. Urol Oncol. 2007;25:110–114. - PubMed
-
- NCCN Clinical Guidelines in Oncology (NCCN Guideline) 2014. Prostate Cancer. Version 1 [Internet]. NCCN; 2014. Available at: http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Accessed January 2014.
-
- Bolla M, van Poppel H, Collette L. Postoperative radiotherapy after radical prostatectomy: a randomised controlled trial (EORTC trial 22911) Lancet. 2005;366:572–578. - PubMed
-
- Thompson IM, Jr, Tangen CM, Paradelo J. Adjuvant radiotherapy for pathologically advanced prostate cancer: a randomized clinical trial. JAMA. 2006;296:2329–2335. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
