

Time to angiographic reperfusion and clinical outcome after acute ischaemic stroke: an analysis of data from the Interventional Management of Stroke (IMS III) phase 3 trial
- PMID: 24784550
- PMCID: PMC4174410
- DOI: 10.1016/S1474-4422(14)70066-3
Time to angiographic reperfusion and clinical outcome after acute ischaemic stroke: an analysis of data from the Interventional Management of Stroke (IMS III) phase 3 trial
Abstract
Background: The IMS III trial did not show a clinical benefit of endovascular treatment compared with intravenous alteplase (recombinant tissue plasminogen activator) alone for moderate or severe ischaemic strokes. Late reperfusion of tissue that was no longer salvageable could be one explanation, as suggested by previous exploratory studies that showed an association between time to reperfusion and good clinical outcome. We sought to validate this association in a preplanned analysis of data from the IMS III trial.
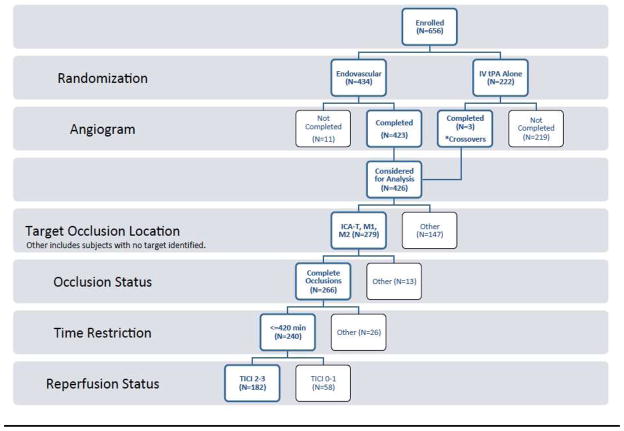
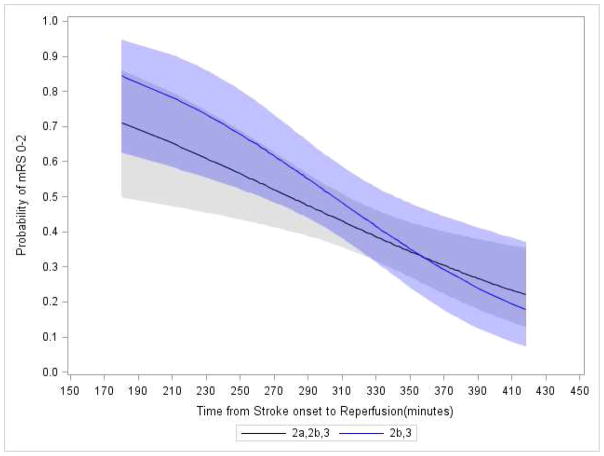
Methods: We used data for patients with complete proximal arterial occlusions in the anterior circulation who received endovascular treatment and achieved angiographic reperfusion (score on Thrombolysis in Cerebral Infarction scale of grade 2-3) during the endovascular procedure (within 7 h of symptom onset). We used logistic regression to model good clinical outcome (defined as a modified Rankin Scale score of 0-2 at 3 months) as a function of the time to reperfusion. We prespecified variables to be considered for adjustment, including age, baseline National Institutes of Health Stroke Scale score, sex, and baseline blood glucose concentration.
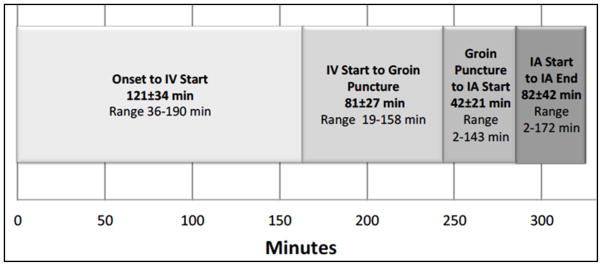
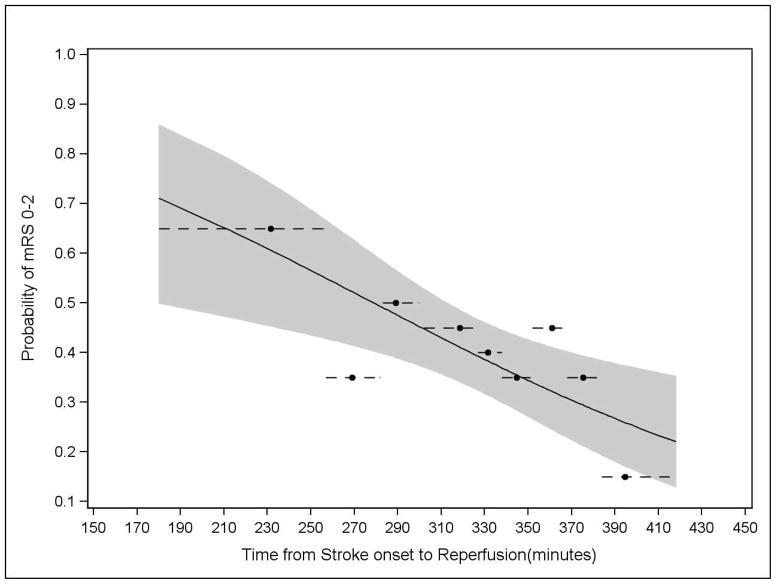
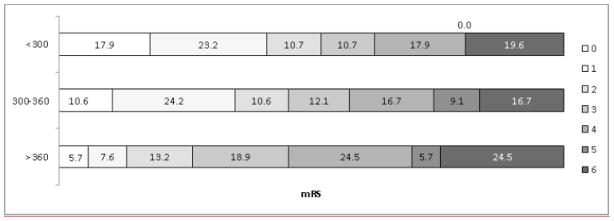
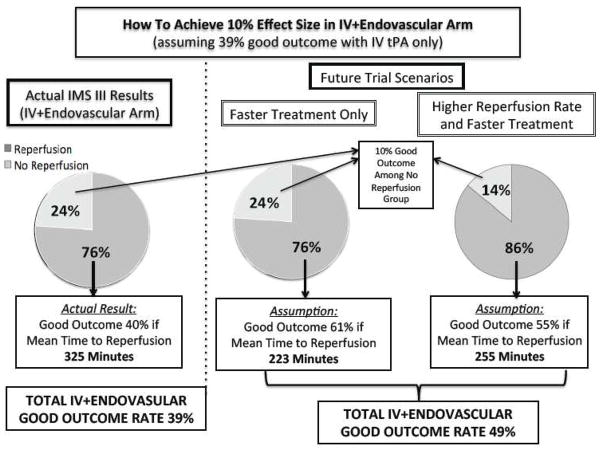
Findings: Of 240 patients who were otherwise eligible for inclusion in our analysis, 182 (76%) achieved angiographic reperfusion. Mean time from symptom onset to reperfusion (ie, procedure end) was 325 min (SD 52). Increased time to reperfusion was associated with a decreased likelihood of good clinical outcome (unadjusted relative risk for every 30-min delay 0·85 [95% CI 0·77-0·94]; adjusted relative risk 0·88 [0·80-0·98]).
Interpretation: Delays in time to angiographic reperfusion lead to a decreased likelihood of good clinical outcome in patients after moderate to severe stroke. Rapid reperfusion could be crucial for the success of future acute endovascular trials.
Funding: US National Institutes of Health and National Institute of Neurological Disorders and Stroke.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Endovascular treatment for stroke: when does the window for good outcome close?Lancet Neurol. 2014 Jun;13(6):529-31. doi: 10.1016/S1474-4422(14)70086-9. Epub 2014 Apr 27. Lancet Neurol. 2014. PMID: 24784551 No abstract available.
-
Complexity of the endovascular intervention and clinical outcomes in acute ischaemic stroke.Lancet Neurol. 2014 Sep;13(9):865. doi: 10.1016/S1474-4422(14)70174-7. Lancet Neurol. 2014. PMID: 25142453 No abstract available.
-
Complexity of the endovascular intervention and clinical outcomes in acute ischaemic stroke--authors' reply.Lancet Neurol. 2014 Sep;13(9):865-6. doi: 10.1016/S1474-4422(14)70175-9. Lancet Neurol. 2014. PMID: 25142454 No abstract available.
References
-
- NINDS rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–7. - PubMed
-
- Broderick JP, Tomsick TA, Palesch YY. Endovascular treatment for acute ischemic stroke. N Engl J Med. 2013;368(25):2432–3. - PubMed
-
- Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375(9727):1695–703. - PubMed
-
- Nogueira RG, Smith WS, Sung G, et al. Effect of Time to Reperfusion on Clinical Outcome of Anterior Circulation Strokes Treated With Thrombectomy: Pooled Analysis of the MERCI and Multi MERCI Trials. Stroke. 2011;42(11):3144–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
