

Association of pulmonary function with adiposity and metabolic abnormalities in urban minority adolescents
- PMID: 24785169
- PMCID: PMC4225805
- DOI: 10.1513/AnnalsATS.201311-403OC
Association of pulmonary function with adiposity and metabolic abnormalities in urban minority adolescents
Abstract
Rationale: Childhood obesity is a known risk factor for pulmonary diseases, likely due to obesity-mediated alteration of pulmonary function. Inflammation and mechanical fat load are two proposed causative mechanisms for altered pulmonary function among obese children; however, the association of metabolic abnormalities with pulmonary function among children is poorly understood.
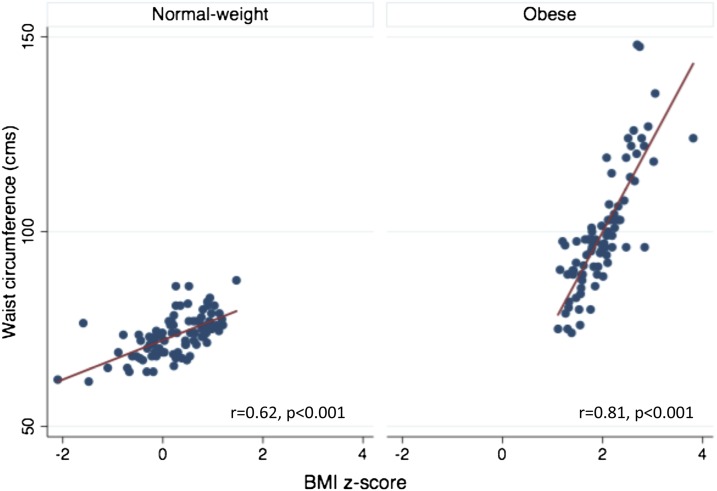
Objectives: We investigated the independent association of truncal and general adiposity and metabolic abnormalities with pulmonary function in a sample of urban minority adolescents.
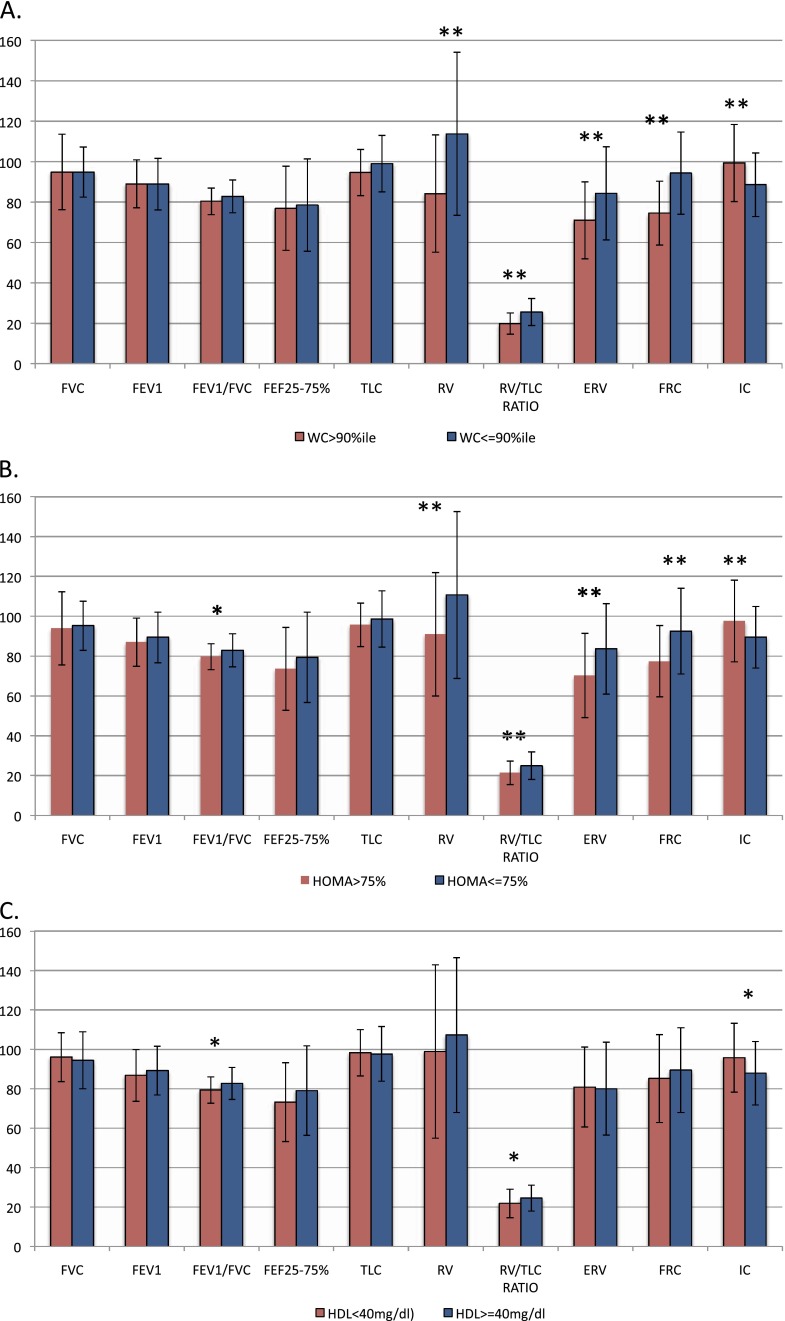
Methods: Spirometry and lung volume indices were compared between adolescents with general (body mass index [BMI] > 95th percentile) or truncal adiposity (waist circumference > 90th percentile) and normal-weight (BMI < 85th percentile or waist circumference ≤ 90th percentile) and between those with metabolic abnormalities (homeostatic model assessment of insulin resistance [HOMA-IR] in the top quartile or high-density lipoprotein [HDL] < 40 mg/dl) and those with a normal metabolic profile.
Measurements and main results: Obese adolescents had lower lung volumes, including residual volume (RV), RV/TLC ratio, expiratory reserve volume (ERV), and FRC, and higher inspiratory capacity (IC) than normal-weight adolescents, but did not differ in measures of lower airway obstruction, FEV1/FVC ratio, and mid-expiratory flow rate. Adolescents with high HOMA-IR had lower FEV1/FVC ratio, RV, RV/TLC ratio, ERV, and FRC and higher IC, whereas those with low HDL had lower FEV1/FVC and RV/TLC ratios. After adjusting for adiposity, HOMA-IR remained a predictor of ERV (β = -1.4; P = 0.02) and FEV1/FVC ratio (β = -0.5; P = 0.03), and HDL remained a predictor of FEV1/FVC ratio (β = 0.1; P = 0.01). General adiposity was a predictor of FRC (β = -0.5; P < 0.001), IC (β = 0.3; P < 0.001), RV (β = -0.8; P < 0.0001), and RV/TLC ratio (β = -0.2; P < 0.0001), and truncal adiposity was a predictor of RV (β = -20.3; P = 0.03) and FRC (β = -13.8; P = 0.004). Thus, adiposity and metabolic abnormalities were independent predictors of ERV, but only metabolic abnormalities independently predicted FEV1/FVC ratio. Although general adiposity predicted RV and RV/TLC ratio, truncal adiposity was predictive of RV and FRC, conferring additional risk above general adiposity.
Conclusions: These results suggest that metabolic abnormalities and adiposity are independently associated with pulmonary function deficits among urban adolescents. Metabolic assessment of obese adolescents may identify those at risk of developing obesity-associated pulmonary morbidity.
Keywords: children; metabolic abnormalities; obesity; pulmonary function.
Figures
References
-
- Dixon AE, Holguin F, Sood A, Salome CM, Pratley RE, Beuther DA, Celedón JC, Shore SA American Thoracic Society Ad Hoc Subcommittee on Obesity and Lung Disease. An official American Thoracic Society Workshop report: obesity and asthma. Proc Am Thorac Soc. 2010;7:325–335. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
