

Diagnosis of childhood tuberculosis and host RNA expression in Africa
- PMID: 24785206
- PMCID: PMC4069985
- DOI: 10.1056/NEJMoa1303657
Diagnosis of childhood tuberculosis and host RNA expression in Africa
Abstract
Background: Improved diagnostic tests for tuberculosis in children are needed. We hypothesized that transcriptional signatures of host blood could be used to distinguish tuberculosis from other diseases in African children who either were or were not infected with the human immunodeficiency virus (HIV).
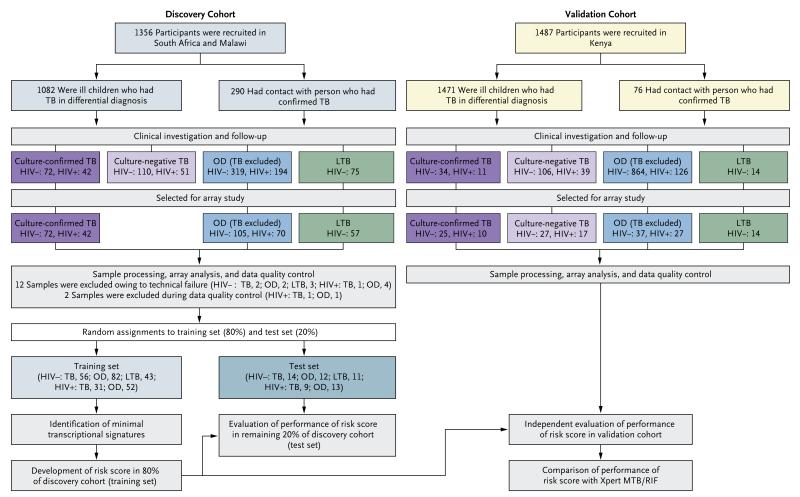
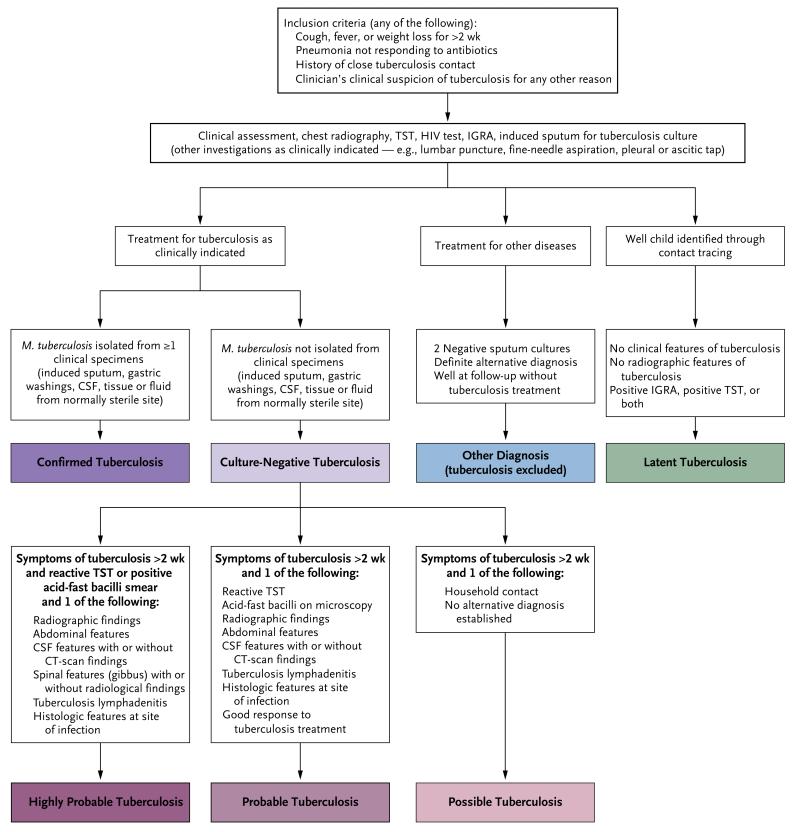
Methods: The study population comprised prospective cohorts of children who were undergoing evaluation for suspected tuberculosis in South Africa (655 children), Malawi (701 children), and Kenya (1599 children). Patients were assigned to groups according to whether the diagnosis was culture-confirmed tuberculosis, culture-negative tuberculosis, diseases other than tuberculosis, or latent tuberculosis infection. Diagnostic signatures distinguishing tuberculosis from other diseases and from latent tuberculosis infection were identified from genomewide analysis of RNA expression in host blood.
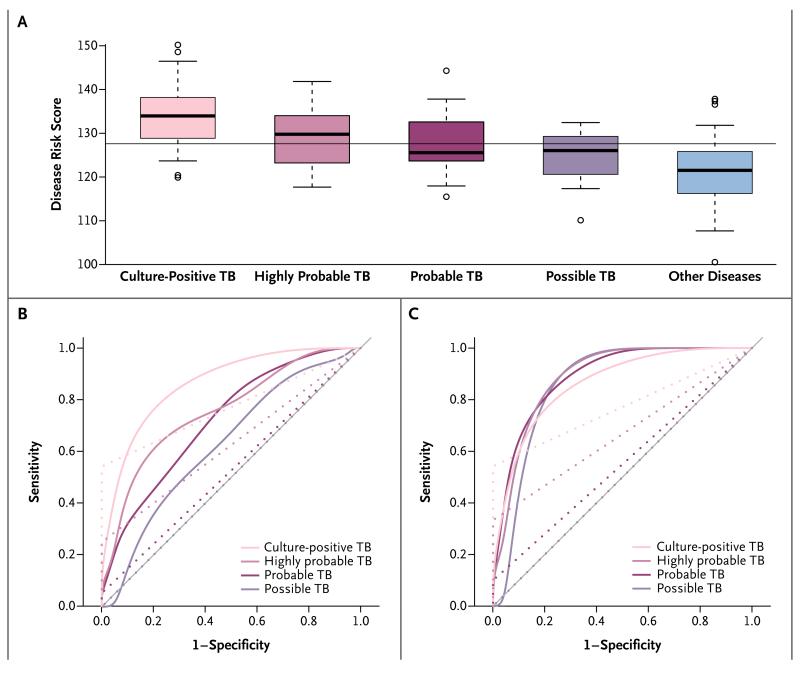
Results: We identified a 51-transcript signature distinguishing tuberculosis from other diseases in the South African and Malawian children (the discovery cohort). In the Kenyan children (the validation cohort), a risk score based on the signature for tuberculosis and for diseases other than tuberculosis showed a sensitivity of 82.9% (95% confidence interval [CI], 68.6 to 94.3) and a specificity of 83.6% (95% CI, 74.6 to 92.7) for the diagnosis of culture-confirmed tuberculosis. Among patients with cultures negative for Mycobacterium tuberculosis who were treated for tuberculosis (those with highly probable, probable, or possible cases of tuberculosis), the estimated sensitivity was 62.5 to 82.3%, 42.1 to 80.8%, and 35.3 to 79.6%, respectively, for different estimates of actual tuberculosis in the groups. In comparison, the sensitivity of the Xpert MTB/RIF assay for molecular detection of M. tuberculosis DNA in cases of culture-confirmed tuberculosis was 54.3% (95% CI, 37.1 to 68.6), and the sensitivity in highly probable, probable, or possible cases was an estimated 25.0 to 35.7%, 5.3 to 13.3%, and 0%, respectively; the specificity of the assay was 100%.
Conclusions: RNA expression signatures provided data that helped distinguish tuberculosis from other diseases in African children with and those without HIV infection. (Funded by the European Union Action for Diseases of Poverty Program and others).
Figures
Comment in
-
Novel biomarkers for paediatric tuberculosis.Lancet Infect Dis. 2014 Oct;14(10):900-1. doi: 10.1016/S1473-3099(14)70898-9. Epub 2014 Aug 31. Lancet Infect Dis. 2014. PMID: 25185460 No abstract available.
References
-
- Perez-Velez CM, Marais BJ. Tuberculosis in children. N Engl J Med. 2012;367:348–61. - PubMed
-
- Global tuberculosis report 2012. World Health Organization; Geneva: 2012.
-
- Zar HJ, Connell TG, Nicol M. Diagnosis of pulmonary tuberculosis in children: new advances. Expert Rev Anti Infect Ther. 2010;8:277–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases