

Sudden unexpected death in epilepsy: knowledge and experience among U.S. and Canadian neurologists
- PMID: 24785429
- PMCID: PMC4176608
- DOI: 10.1016/j.yebeh.2014.03.022
Sudden unexpected death in epilepsy: knowledge and experience among U.S. and Canadian neurologists
Abstract
Importance: Sudden unexpected death in epilepsy (SUDEP) is a common cause of mortality in patients with the disease, but it is unknown how neurologists disclose this risk when counseling patients.
Objective: This study aimed at examining SUDEP discussion practices of neurologists in the U.S. and Canada.
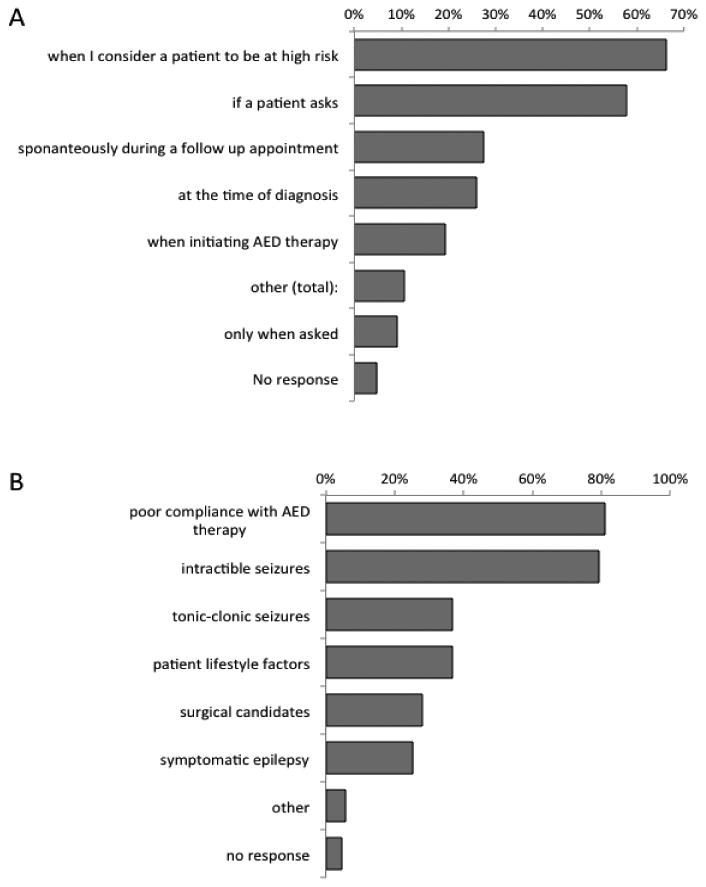
Design: An electronic, web-based survey was sent to 17,558 neurologists in the U.S. and Canada. Survey questions included frequency of SUDEP discussion, reasons for discussing/not discussing SUDEP, timing of SUDEP discussions, and perceived patient reactions. We examined factors that influence the frequency of SUDEP discussion and perceived patient response using multivariate logistic regression.
Participants: The participants of this study were neurologists who completed postgraduate training and devoted >5% of their time to patient care.
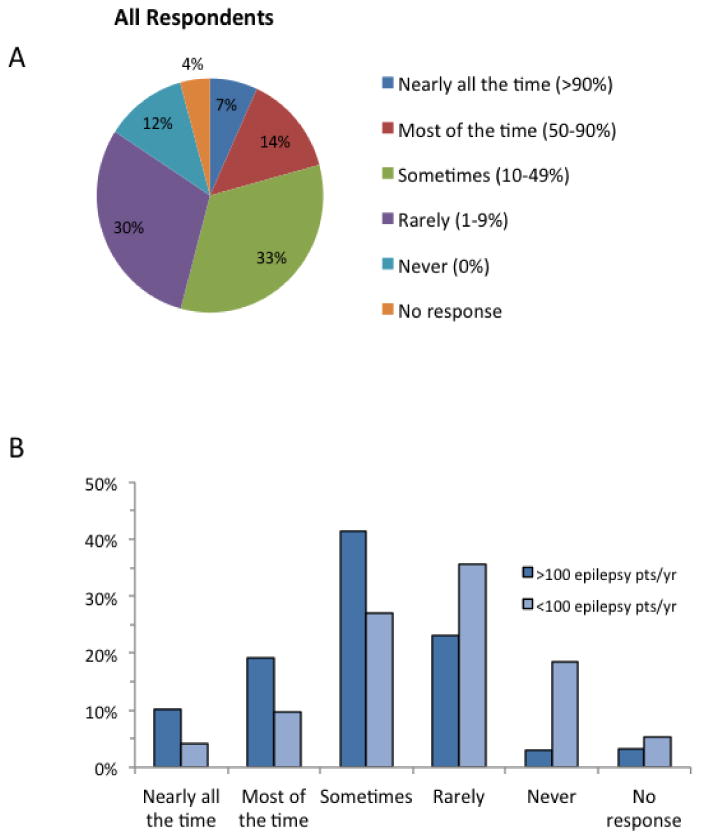
Results: There was a response rate of 9.3%; 1200 respondents met eligibility criteria and completed surveys. Only 6.8% of the respondents discussed SUDEP with nearly all (>90% of the time) of their patients with epilepsy/caregivers, while 11.6% never discussed it. Factors that independently predicted whether SUDEP was discussed nearly all of the time were the following: number of patients with epilepsy seen annually (OR=2.01, 95% CI=1.20-3.37, p<0.01) and if the respondent had a SUDEP case in the past 24 months (OR=2.27, 95% CI=1.37-3.66, p<0.01). A majority of respondents (59.5%) reported that negative reactions were the most common response to a discussion of SUDEP. Having additional epilepsy/neurophysiology training was associated with an increased risk of a perceived negative response (OR=1.36, 95% CI=1.02-1.82, p=0.038), while years in practice (OR=0.85, 95% CI=0.77-0.95, p<0.005) and seeing both adults and children were associated with a decreased likelihood of negative response (OR=0.15, 95% CI=0.032-0.74, p=0.02).
Conclusions: U.S. and Canadian neurologists rarely discuss SUDEP with all patients with epilepsy/caregivers though discussions are more likely among neurologists who frequently see patients with epilepsy or had a recent SUDEP in their practice. Perceived negative reactions to SUDEP discussions are common but not universal; more experienced neurologists may be less likely to encounter negative reactions, suggesting that there may be ways to frame the discussion that minimizes patient/caregiver distress.
Keywords: Counseling; Disclosure; Education; SUDEP.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Devinsky O. Sudden, unexpected death in epilepsy. The New England journal of medicine. 2011;365:1801–11. - PubMed
-
- Nashef L. Sudden Unexpected Death in Epilepsy: Terminology and Definitions. Epilepsia. 1997;38:S6–S8. - PubMed
-
- Tomson T, Nashef L, Ryvlin P. Sudden unexpected death in epilepsy: current knowledge and future directions. Lancet Neurology. 2008;7:1021–31. - PubMed
-
- Hesdorffer DC, Tomson T, Benn E, Sander JW, Nilsson L, Langan Y, Walczak TS, Beghi E, Brodie MJ, Hauser A. Combined analysis of risk factors for SUDEP. Epilepsia. 2011;52:1150–9. - PubMed
-
- National Institute for Health and Clinical Excellence. The diagnosis and management of the epilepsies in adults and children in primary and secondary care. 2007 CG20.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
