

Current status in the therapy of liver diseases
- PMID: 24786290
- PMCID: PMC4057686
- DOI: 10.3390/ijms15057500
Current status in the therapy of liver diseases
Abstract
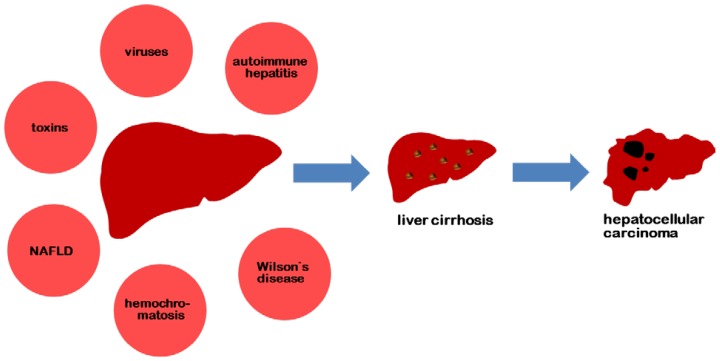
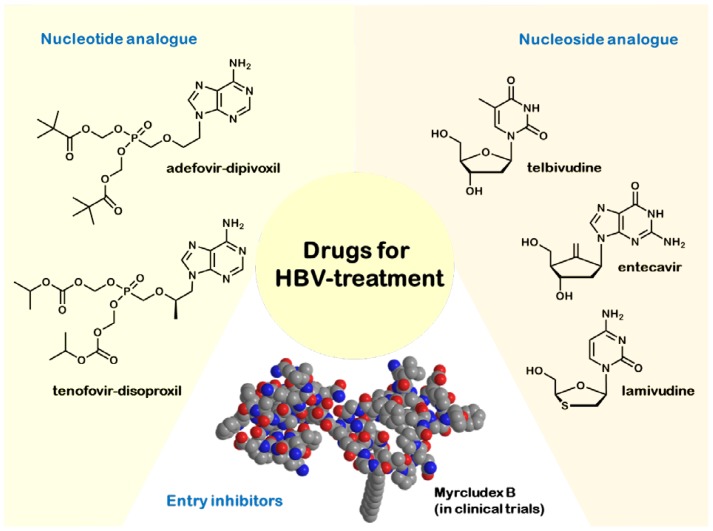
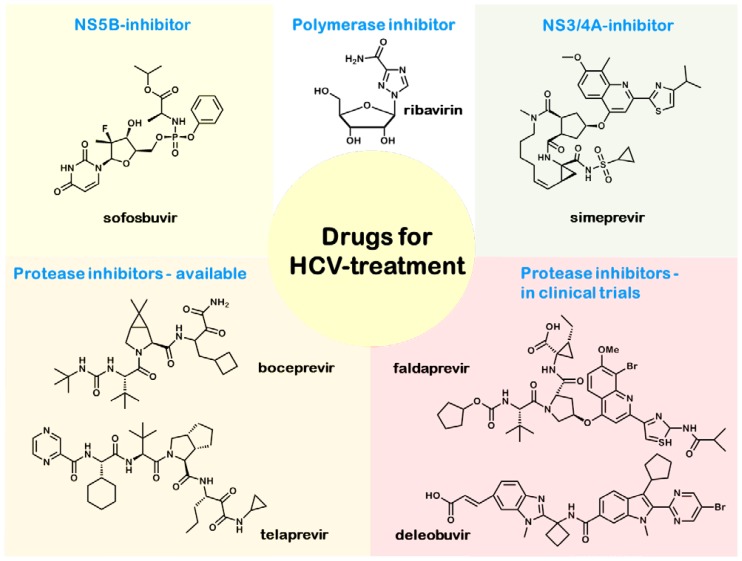
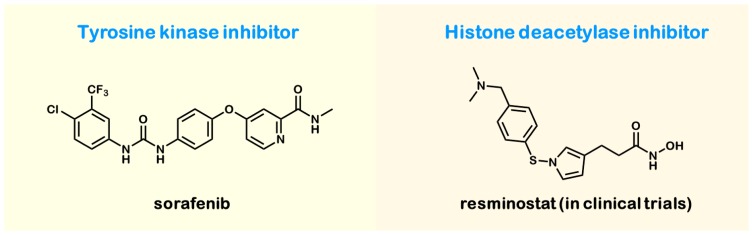
Hepatic diseases, like viral hepatitis, autoimmune hepatitis, hereditary hemochromatosis, non-alcoholic fatty liver disease (NAFLD) and Wilson's disease, play an important role in the development of liver cirrhosis and, hence, hepatocellular carcinoma. In this review, the current treatment options and the molecular mechanisms of action of the drugs are summarized. Unfortunately, the treatment options for most of these hepatic diseases are limited. Since hepatitis B (HBV) and C (HCV) infections are the most common causes of liver cirrhosis and hepatocellular carcinoma, they are the focus of the development of new drugs. The current treatment of choice for HBV/HCV infection is an interferon-based combination therapy with oral antiviral drugs, like nucleos(t)ide analogues, which is associated with improving the therapeutic success and also preventing the development of resistances. Currently, two new protease inhibitors for HCV treatment are expected (deleobuvir, faldaprevir) and together with the promising drug, daclatasvir (NS5A-inhibitor, currently in clinical trials), adequate therapy is to be expected in due course (circumventing the requirement of interferon with its side-effects), while in contrast, efficient HBV therapeutics are still lacking. In this respect, entry inhibitors, like Myrcludex B, the lead substance of the first entry inhibitor for HBV/HDV (hepatitis D) infection, provide immense potential. The pharmacokinetics and the mechanism of action of Myrcludex B are described in detail.
Figures
References
-
- Rehermann B., Nascimbeni M. Immunology of hepatitis B virus and hepatitis C virus infection. Nat. Rev. Immunol. 2005;5:215–229. - PubMed
-
- Perz J.F., Armstrong G.L., Farrington L.A., Hutin Y.J., Bell B.P. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J. Hepatol. 2006;45:529–538. - PubMed
-
- Desmet V.J., Gerber M., Hoofnagle J.H., Manns M., Scheuer P.J. Classification of chronic hepatitis: Diagnosis, grading and staging. Hepatology. 1994;19:1513–1520. - PubMed
-
- Van Herck K., van Damme P. Prevention of hepatitis A by Havrix™: A review. Expert Rev. Vaccines. 2005;4:459–471. - PubMed
-
- Böttcher B., Wynne S.A., Crowther R.A. Determination of the fold of the core protein of hepatitis B virus by electron cryomicroscopy. Nature. 1997;386:88–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
