

An acellular biologic scaffold promotes skeletal muscle formation in mice and humans with volumetric muscle loss
- PMID: 24786326
- PMCID: PMC5942588
- DOI: 10.1126/scitranslmed.3008085
An acellular biologic scaffold promotes skeletal muscle formation in mice and humans with volumetric muscle loss
Abstract
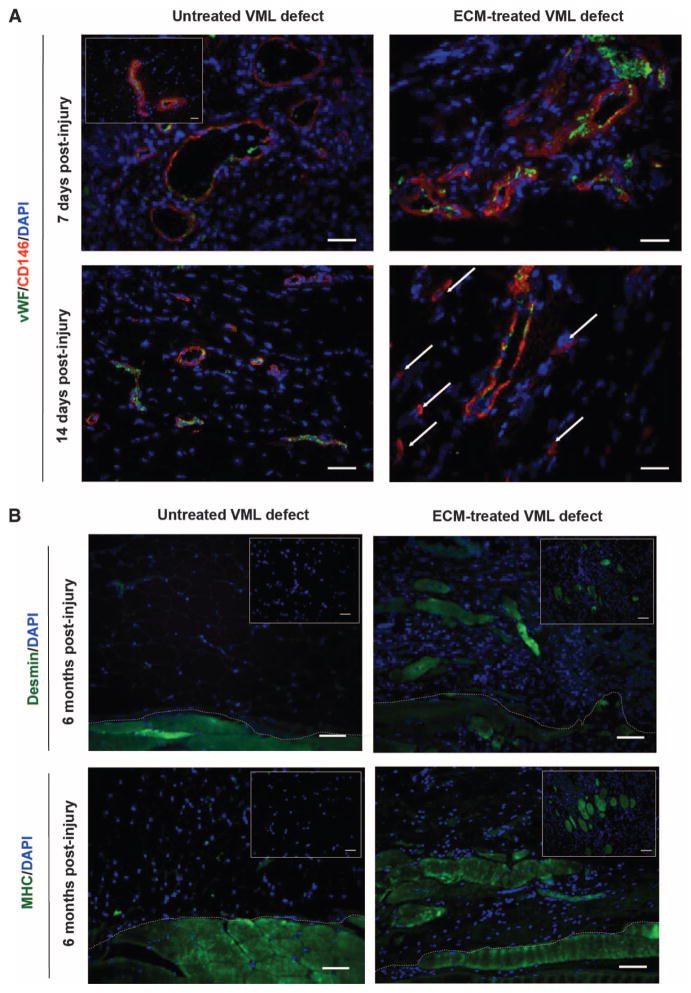
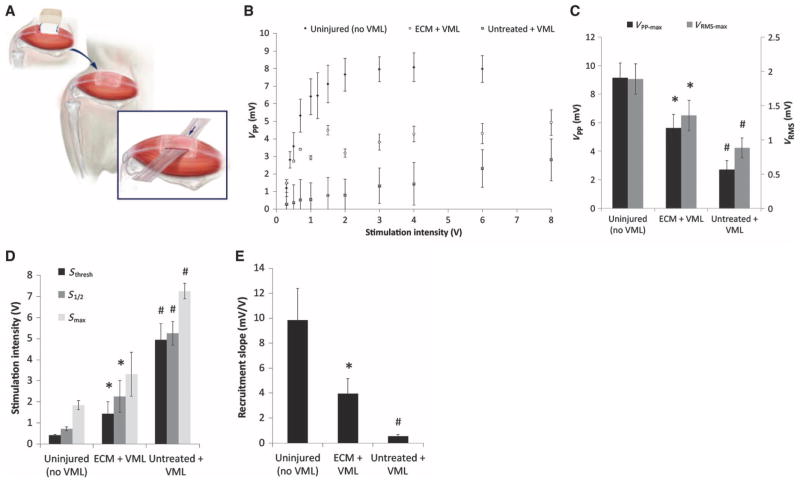
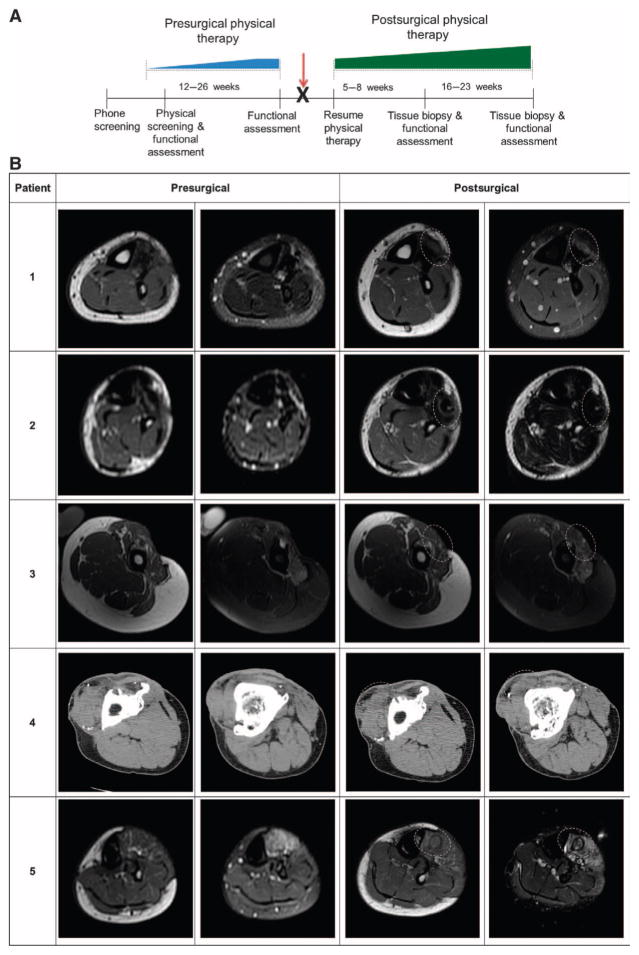
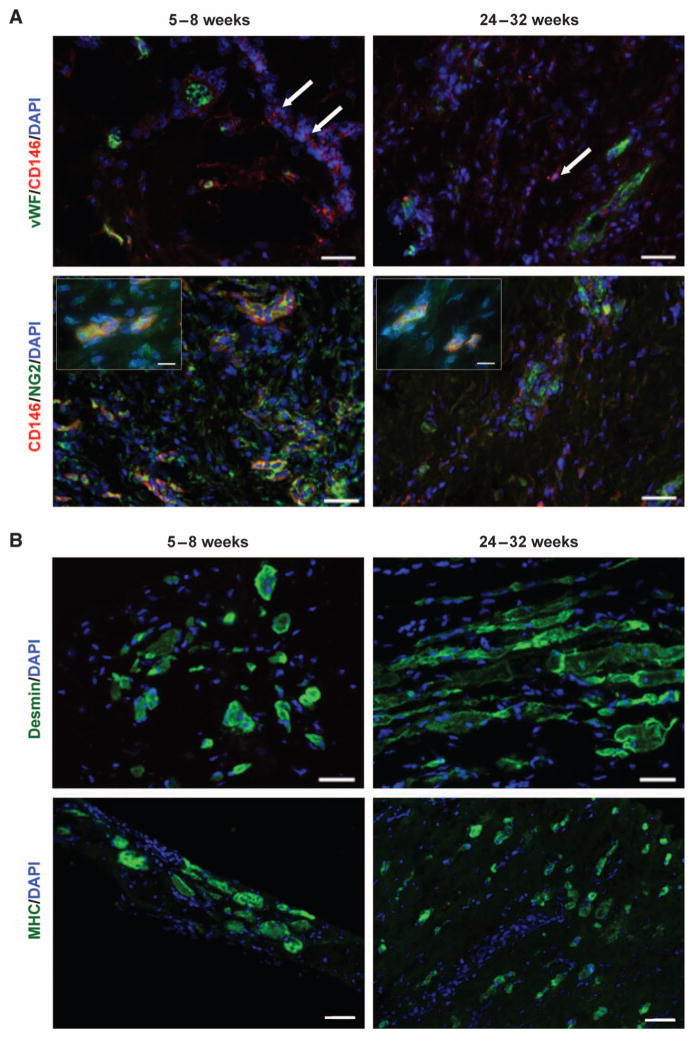
Biologic scaffolds composed of naturally occurring extracellular matrix (ECM) can provide a microenvironmental niche that alters the default healing response toward a constructive and functional outcome. The present study showed similarities in the remodeling characteristics of xenogeneic ECM scaffolds when used as a surgical treatment for volumetric muscle loss in both a preclinical rodent model and five male patients. Porcine urinary bladder ECM scaffold implantation was associated with perivascular stem cell mobilization and accumulation within the site of injury, and de novo formation of skeletal muscle cells. The ECM-mediated constructive remodeling was associated with stimulus-responsive skeletal muscle in rodents and functional improvement in three of the five human patients.
Conflict of interest statement
Figures
References
-
- Huard J, Li Y, Fu FH. Muscle injuries and repair: Current trends in research. J Bone Joint Surg Am. 2002;84-A:822–832. - PubMed
-
- Chargé SB, Rudnicki MA. Cellular and molecular regulation of muscle regeneration. Physiol Rev. 2004;84:209–238. - PubMed
-
- Järvinen T, Järvinen TL, Kääriäinen M, Kalimo H, Järvinen M. Muscle injuries: Biology and treatment. Am J Sports Med. 2005;33:745–764. - PubMed
-
- Carlson BM, Faulkner JA. The regeneration of skeletal muscle fibers following injury: A review. Med Sci Sports Exerc. 1983;15:187–198. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
