

An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease
- PMID: 24787074
- PMCID: PMC4098112
- DOI: 10.1164/rccm.201402-0373ST
An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease
Abstract
Background: Limb muscle dysfunction is prevalent in chronic obstructive pulmonary disease (COPD) and it has important clinical implications, such as reduced exercise tolerance, quality of life, and even survival. Since the previous American Thoracic Society/European Respiratory Society (ATS/ERS) statement on limb muscle dysfunction, important progress has been made on the characterization of this problem and on our understanding of its pathophysiology and clinical implications.
Purpose: The purpose of this document is to update the 1999 ATS/ERS statement on limb muscle dysfunction in COPD.
Methods: An interdisciplinary committee of experts from the ATS and ERS Pulmonary Rehabilitation and Clinical Problems assemblies determined that the scope of this document should be limited to limb muscles. Committee members conducted focused reviews of the literature on several topics. A librarian also performed a literature search. An ATS methodologist provided advice to the committee, ensuring that the methodological approach was consistent with ATS standards.
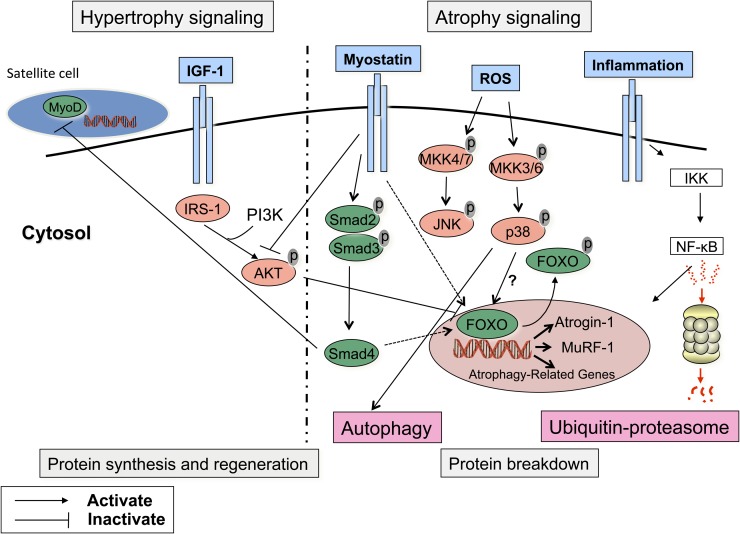
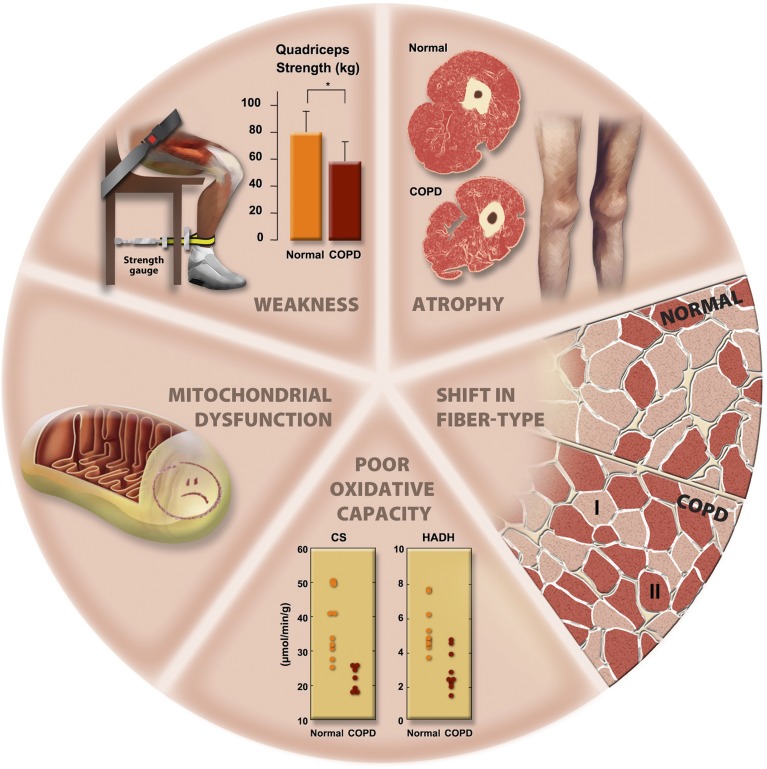
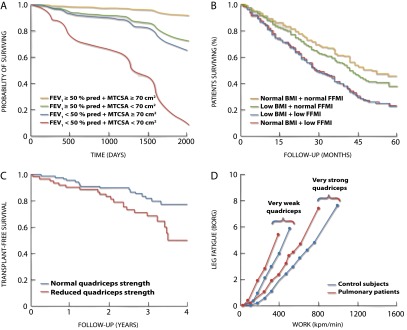
Results: We identified important advances in our understanding of the extent and nature of the structural alterations in limb muscles in patients with COPD. Since the last update, landmark studies were published on the mechanisms of development of limb muscle dysfunction in COPD and on the treatment of this condition. We now have a better understanding of the clinical implications of limb muscle dysfunction. Although exercise training is the most potent intervention to address this condition, other therapies, such as neuromuscular electrical stimulation, are emerging. Assessment of limb muscle function can identify patients who are at increased risk of poor clinical outcomes, such as exercise intolerance and premature mortality.
Conclusions: Limb muscle dysfunction is a key systemic consequence of COPD. However, there are still important gaps in our knowledge about the mechanisms of development of this problem. Strategies for early detection and specific treatments for this condition are also needed.
Figures

References
-
- Skeletal muscle dysfunction in chronic obstructive pulmonary disease: a statement of the American Thoracic Society and European Respiratory Society. Am J Respir Crit Care Med. 1999;159:S1–S40. - PubMed
-
- Evans WJ, Morley JE, Argilés J, Bales C, Baracos V, Guttridge D, Jatoi A, Kalantar-Zadeh K, Lochs H, Mantovani G, et al. Cachexia: a new definition. Clin Nutr. 2008;27:793–799. - PubMed
-
- Burke RE. Revisiting the notion of ‘motor unit types.’. Prog Brain Res. 1999;123:167–175. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
