

Effects of sex on coronary microvascular dysfunction and cardiac outcomes
- PMID: 24787469
- PMCID: PMC4076200
- DOI: 10.1161/CIRCULATIONAHA.113.008507
Effects of sex on coronary microvascular dysfunction and cardiac outcomes
Abstract
Background: Coronary microvascular dysfunction (CMD) is a prevalent and prognostically important finding in patients with symptoms suggestive of coronary artery disease. The relative extent to which CMD affects both sexes is largely unknown.
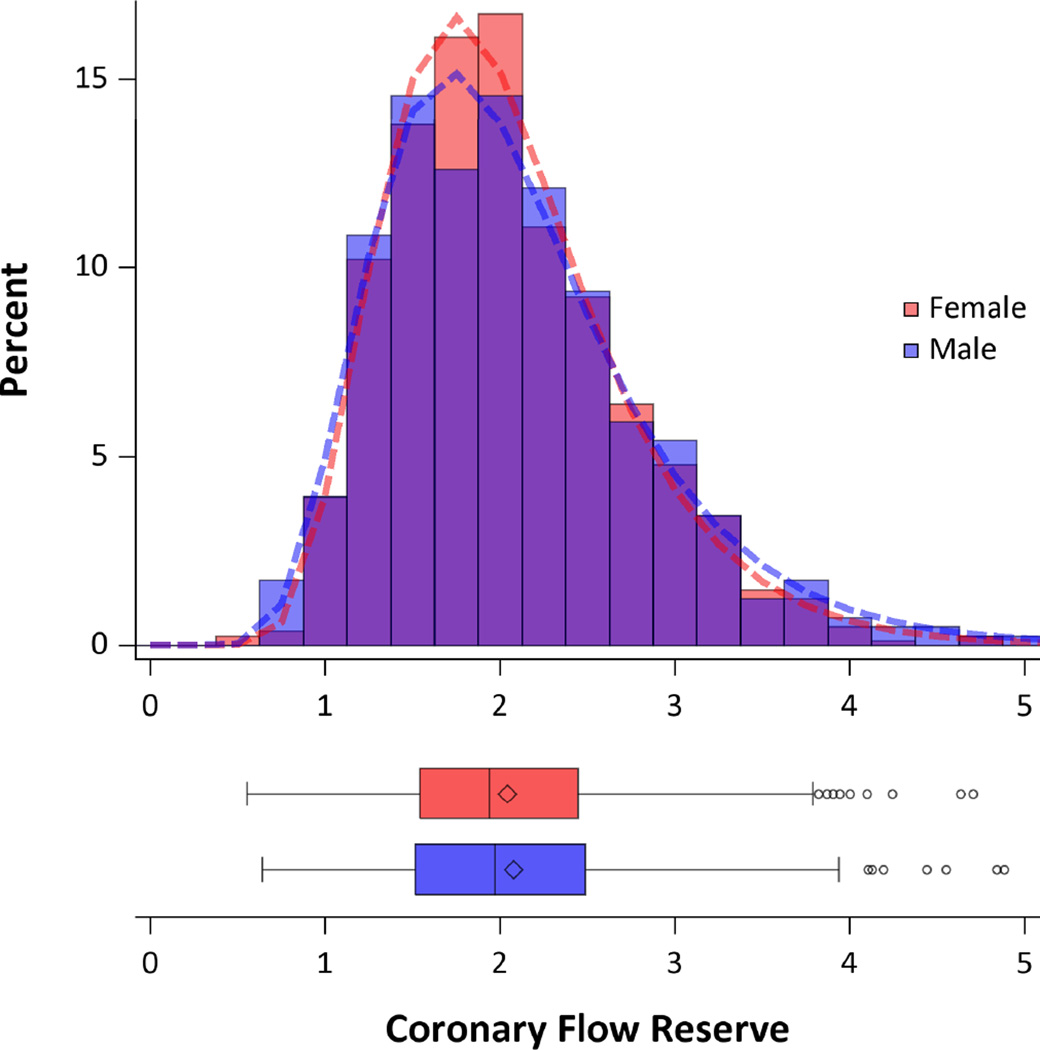
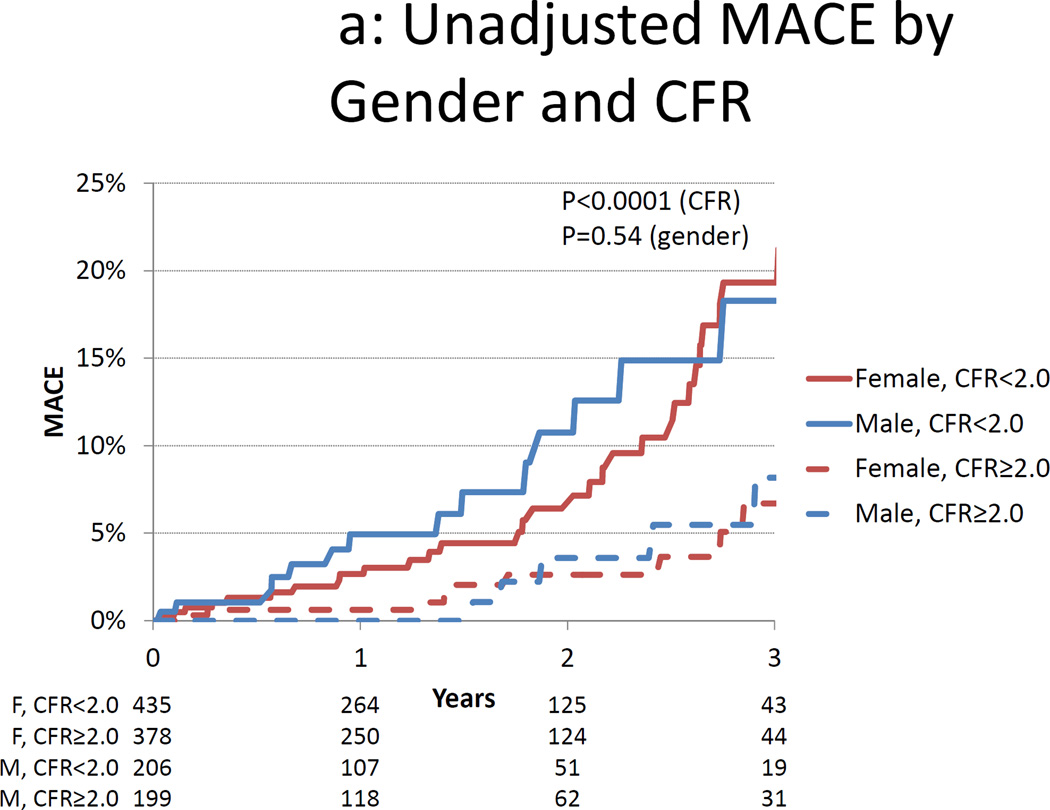
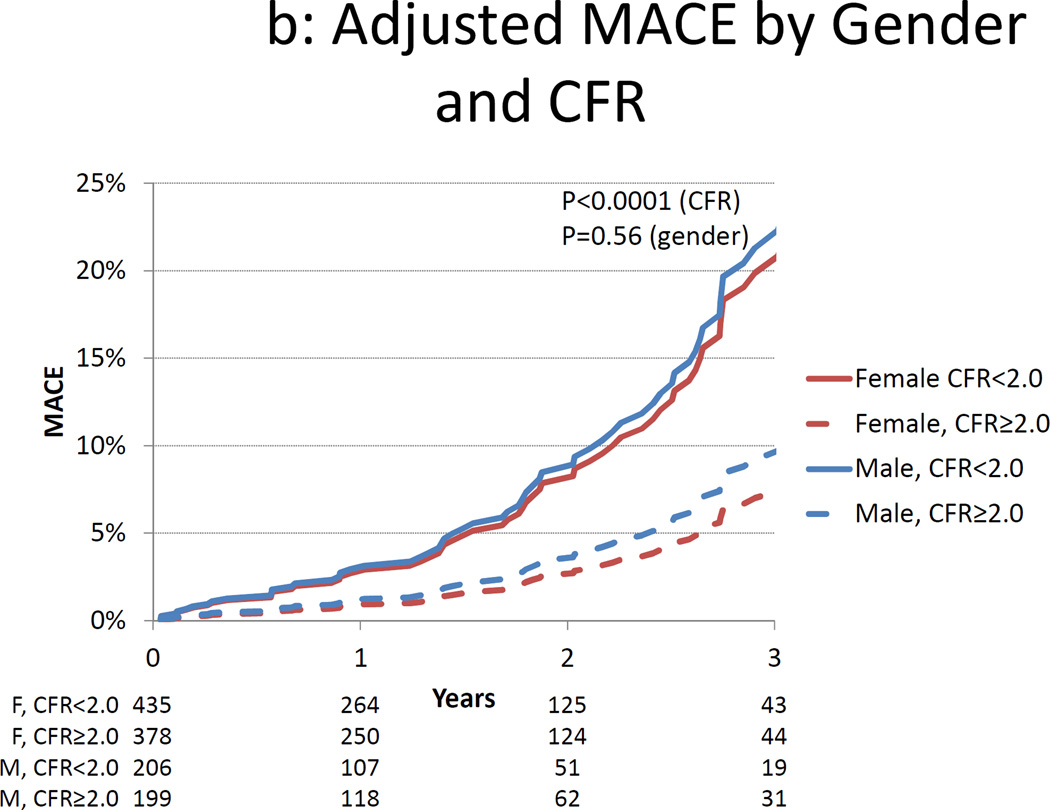
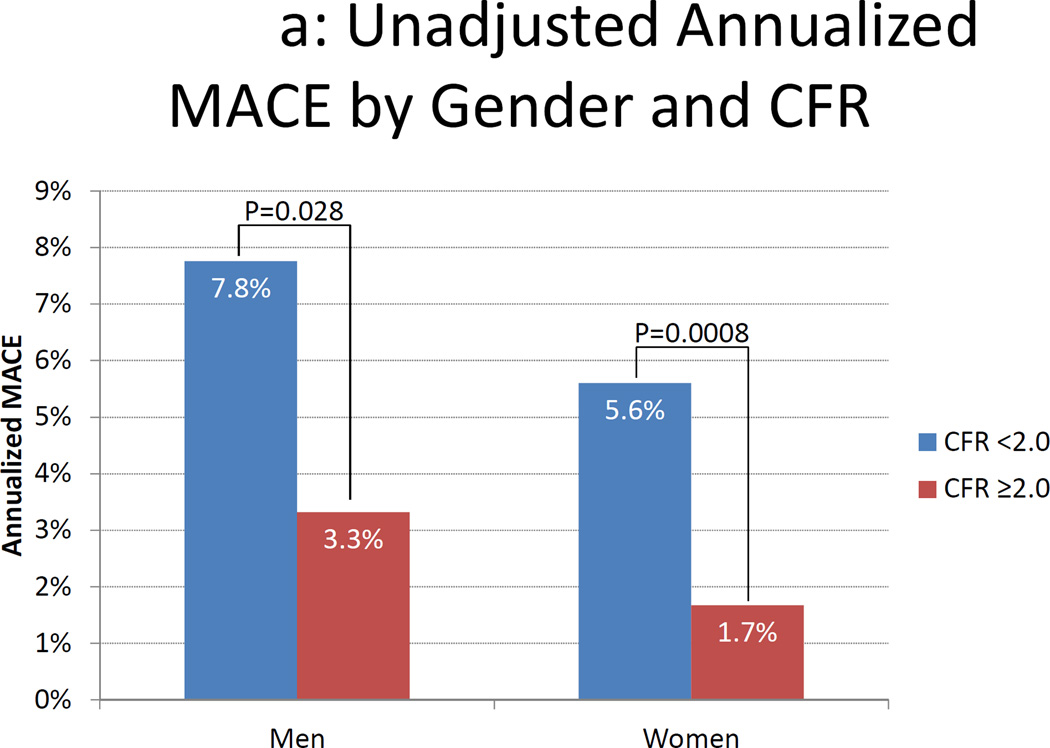
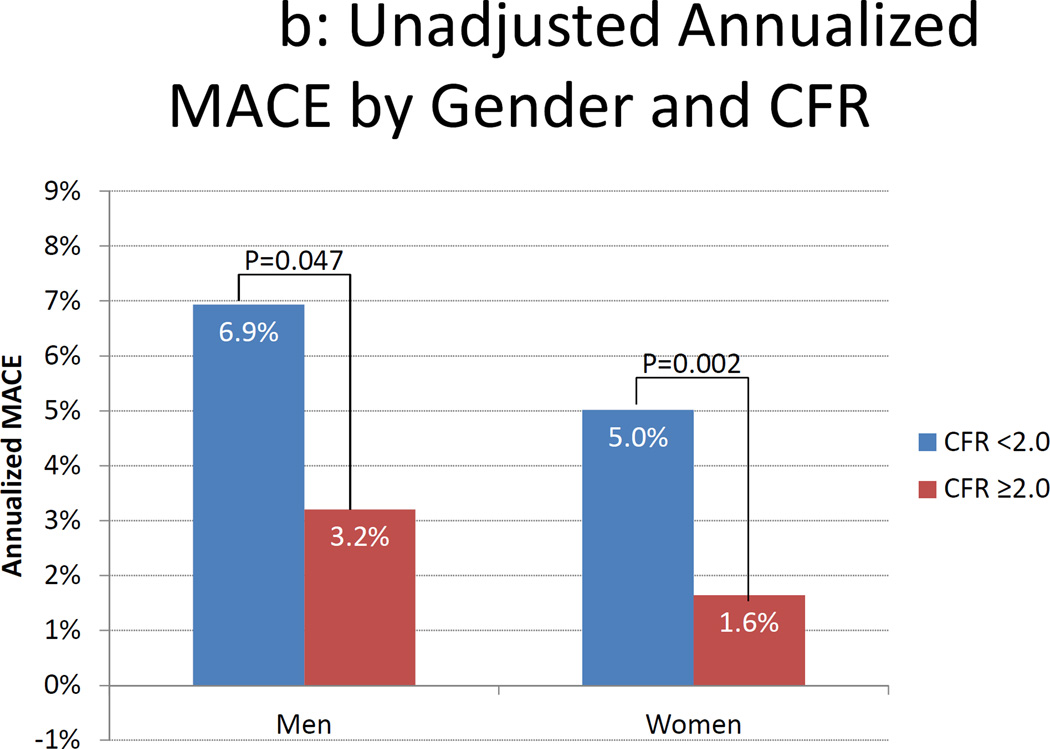
Methods and results: We investigated 405 men and 813 women who were referred for evaluation of suspected coronary artery disease with no previous history of coronary artery disease and no visual evidence of coronary artery disease on rest/stress positron emission tomography myocardial perfusion imaging. Coronary flow reserve was quantified, and coronary flow reserve <2.0 was used to define the presence of CMD. Major adverse cardiac events, including cardiac death, nonfatal myocardial infarction, late revascularization, and hospitalization for heart failure, were assessed in a blinded fashion over a median follow-up of 1.3 years (interquartile range, 0.5-2.3 years). CMD was highly prevalent both in men and women (51% and 54%, respectively; Fisher exact test =0.39; equivalence P=0.0002). Regardless of sex, coronary flow reserve was a powerful incremental predictor of major adverse cardiac events (hazard ratio, 0.80 [95% confidence interval, 0.75-086] per 10% increase in coronary flow reserve; P<0.0001) and resulted in favorable net reclassification improvement (0.280 [95% confidence interval, 0.049-0.512]), after adjustment for clinical risk and ventricular function. In a subgroup (n=404; 307 women/97 men) without evidence of coronary artery calcification on gated computed tomography imaging, CMD was common in both sexes, despite normal stress perfusion imaging and no coronary artery calcification (44% of men versus 48% of women; Fisher exact test P=0.56; equivalence P=0.041).
Conclusions: CMD is highly prevalent among at-risk individuals and is associated with adverse outcomes regardless of sex. The high prevalence of CMD in both sexes suggests that it may be a useful target for future therapeutic interventions.
Keywords: atherosclerosis; blood flow velocity; microcirculation; sex; women.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Figures
Comment in
-
The prevalence of microvascular dysfunction, its role among men, and links with adverse outcomes: noninvasive imaging reveals the tip of the iceberg.Circulation. 2014 Jun 17;129(24):2497-9. doi: 10.1161/CIRCULATIONAHA.114.010263. Epub 2014 Apr 30. Circulation. 2014. PMID: 24787470 Free PMC article. No abstract available.
-
Letter by Galyfos and Filis regarding article, "effects of sex on coronary microvascular dysfunction and cardiac outcomes".Circulation. 2015 Mar 17;131(11):e375. doi: 10.1161/CIRCULATIONAHA.114.011642. Circulation. 2015. PMID: 25779547 No abstract available.
-
Response to letter regarding article, "effects of sex on coronary microvascular dysfunction and cardiac outcomes".Circulation. 2015 Mar 17;131(11):e376. doi: 10.1161/CIRCULATIONAHA.114.012827. Circulation. 2015. PMID: 25779548 No abstract available.
References
-
- Kennedy JW, Killip T, Fisher LDP, Alderman EL, Gillespie MJ, Mock MB., III The clinical spectrum of coronary artery disease and its surgical and medical management, 1974–1979. The Coronary Artery Surgery study. Circulation. 1982;66:16–23. - PubMed
-
- McClelland RL, Chung H, Detrano R, Post W, Kronmal RA. Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA) Circulation. 2006;113:30–37. - PubMed
-
- Johnson BD, Shaw LJ, Buchthal SD, Bairey Merz CN, Kim H-W, Scott KN, Doyle M, Olson MB, Pepine CJ, den Hollander J, Sharaf B, Rogers WJ, Mankad S, Forder JR, Kelsey SF, Pohost GM. Prognosis in women with myocardial ischemia in the absence of obstructive coronary disease: results from the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE) Circulation. 2004;109:2993–2999. - PubMed
-
- Pepine CJ, Anderson RD, Sharaf BL, Reis SE, Smith KM, Handberg EM, Johnson BD, Sopko G, Bairey Merz CN. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women’s Ischemia Syndrome Evaluation) study. J Am Coll Cardiol. 2010;55:2825–2832. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
