

A comparative effectiveness analysis of visual field outcomes after projected glaucoma screening using SD-OCT in African American communities
- PMID: 24787570
- PMCID: PMC4073998
- DOI: 10.1167/iovs.14-14014
A comparative effectiveness analysis of visual field outcomes after projected glaucoma screening using SD-OCT in African American communities
Abstract
Purpose: To assess the impact on visual function of community glaucoma screening in an African American population using spectral-domain optical coherence tomography (SD-OCT).
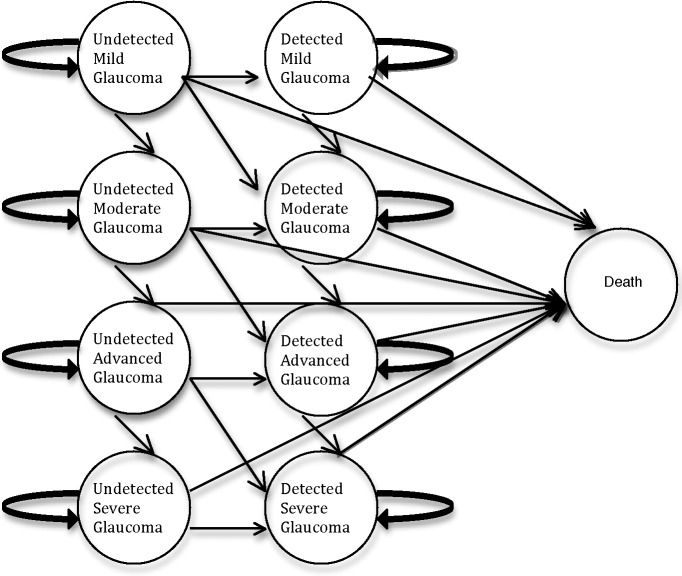
Methods: Using a Monte Carlo microsimulation model with a 10-year time horizon, we analyzed the efficacy of SD-OCT screening on visual field outcomes in a population of African Americans who are not otherwise seeking office-based care. Outcomes included classification of visual field severity, quality-adjusted life years, and direct health care costs.
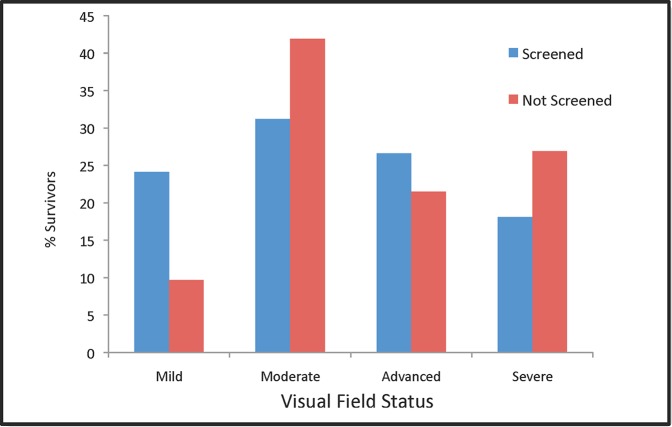
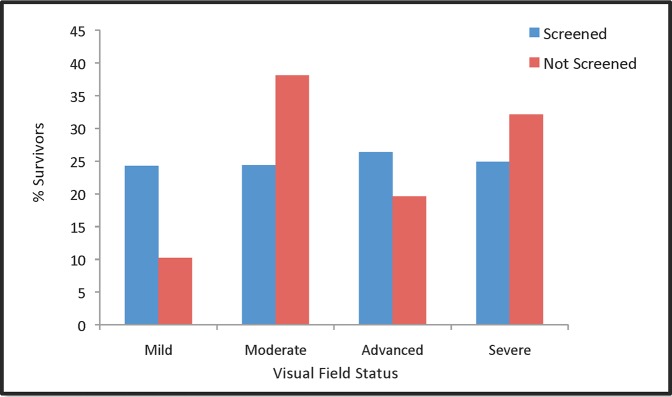
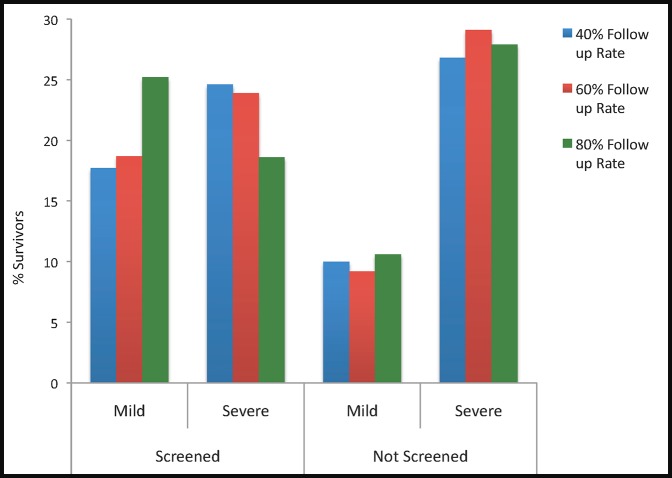
Results: Assuming a 60% follow-up rate, screening decreased the prevalence of undiagnosed glaucoma from 75% to 38%, and decreased the prevalence of severe visual field loss in patients with glaucoma from 29.1% to 23.9%. Conversely, screening increased the prevalence of mild visual field loss in patients with glaucoma from 9.2% to 18.7%. From initial screening through confirmatory eye examination, the screening program ("screen only") cost $98 per screened individual, and $2561 per new diagnosis of glaucoma. When considering the costs of initial screening though the resultant treatment, the screening program ("screen and treat") had an average annual cost of $79 and $2138, respectively, over a 10-year time period. The cost of one quality-adjusted life year (QALY) gained by screening, including management and treatment, in comparison with opportunistic case finding, ranged from $46,416 to $67,813.
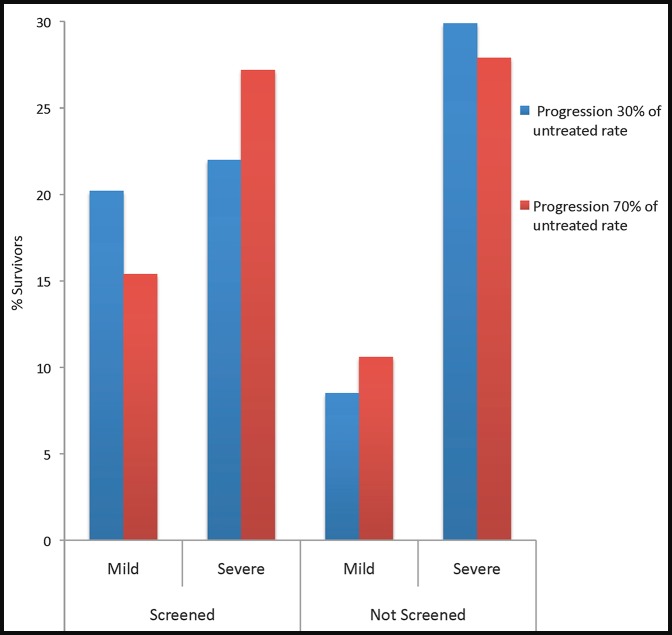
Conclusions: Our findings suggest that community SD-OCT screening in an African American population will minimize glaucoma-related visual morbidity. Ideally, strategies to maximize treatment efficacy through improved medication adherence and improved compliance with follow-up should be identified and implemented before instituting a screening program.
Keywords: Markov model; SD-OCT; comparative effectiveness; glaucoma; screening.
Copyright 2014 The Association for Research in Vision and Ophthalmology, Inc.
Figures
References
-
- Tielsch JM, Sommer A, Katz J, Royall RM, Quigley H, Javitt J. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA. 1991; 266: 369–374 - PubMed
-
- Varma R, Ying-Lai M, Francis BA, et al. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: the Los Angeles Latino Eye Study. Ophthalmology. 2004; 111: 1439–1448 - PubMed
-
- Muñoz B, West SK, Rubin GS, et al. Causes of blindness and visual impairment in a population of older Americans: the Salisbury Eye Evaluation Study. Arch Ophthalmol. 2000; 118: 819–825 - PubMed
-
- Fleming C, Whitlock E, Beil T, Smit B. Primary Care Screening for Ocular Hypertension and Primary Open-Angle Glaucoma. Agency for Healthcare Research and Quality (US): Rockville; 2005. Available at: Accessed February, 16 2013. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
