

An integrated computational model of the bone microenvironment in bone-metastatic prostate cancer
- PMID: 24788098
- PMCID: PMC4023121
- DOI: 10.1158/0008-5472.CAN-13-2652
An integrated computational model of the bone microenvironment in bone-metastatic prostate cancer
Abstract
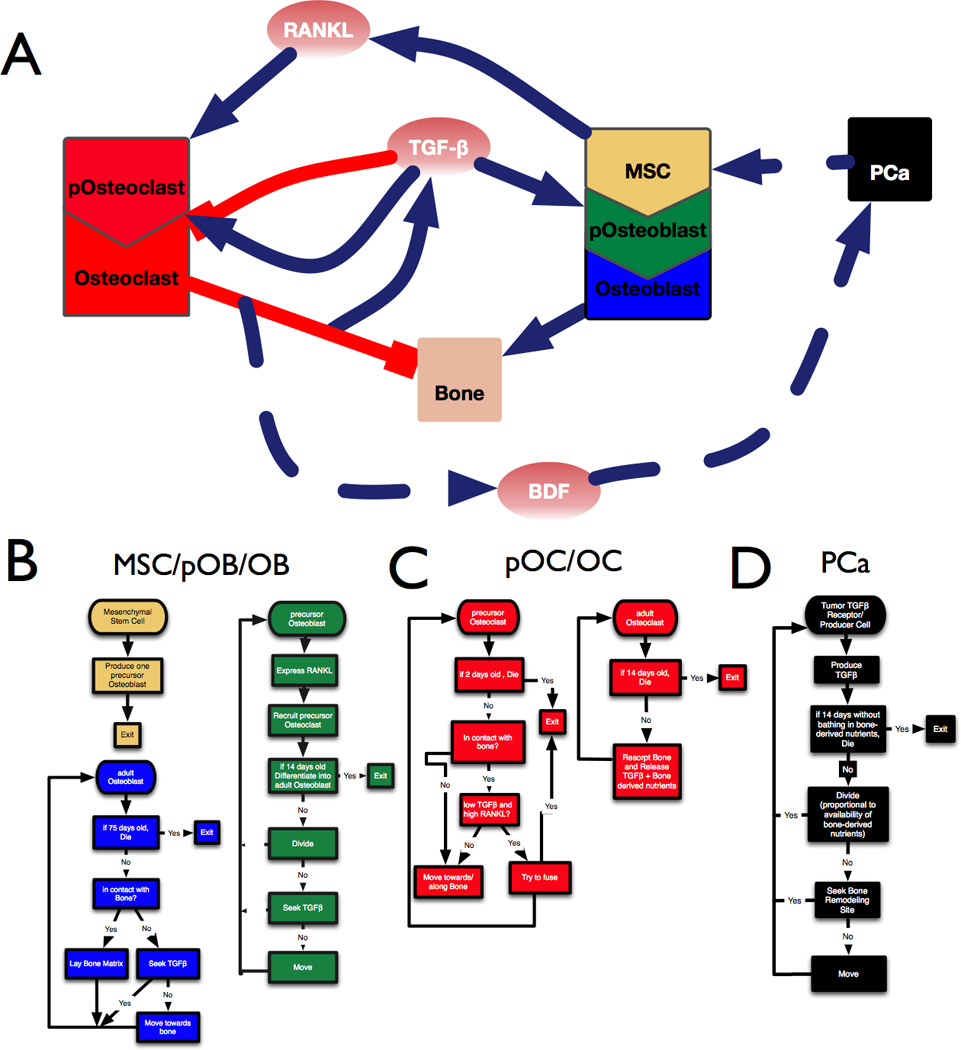
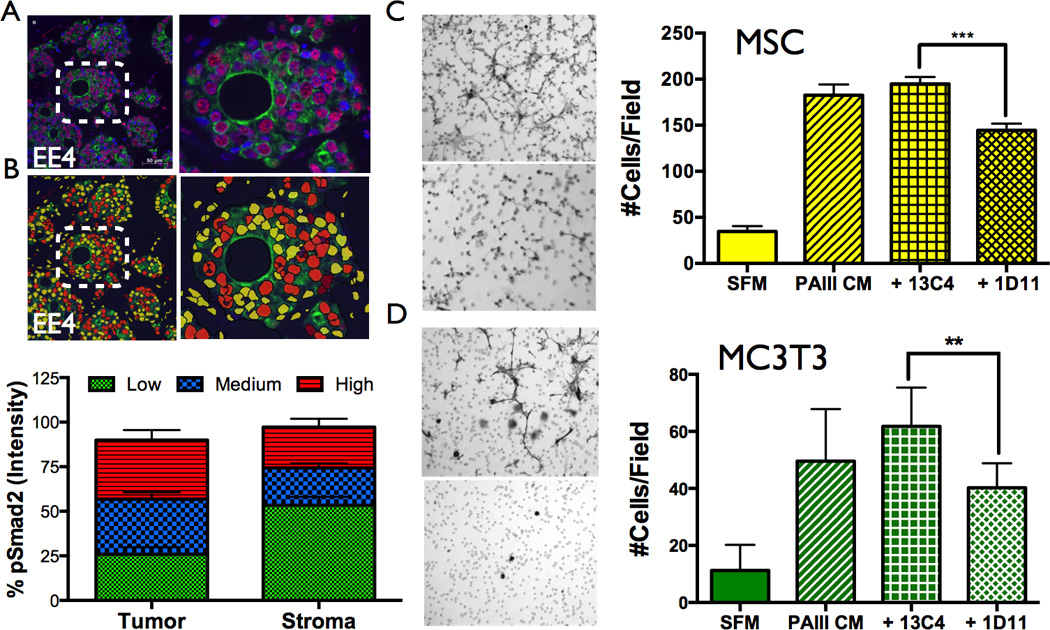
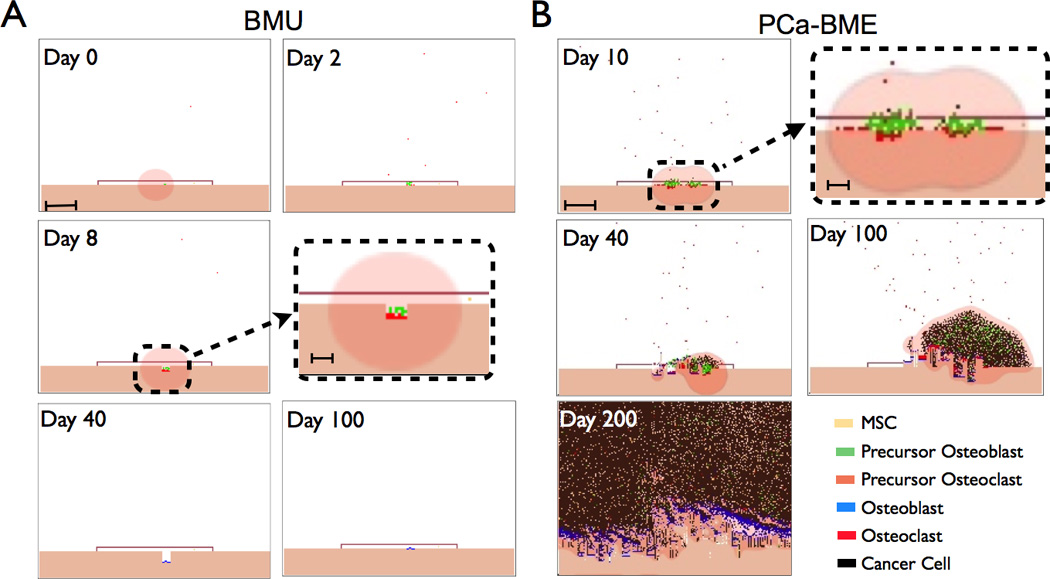
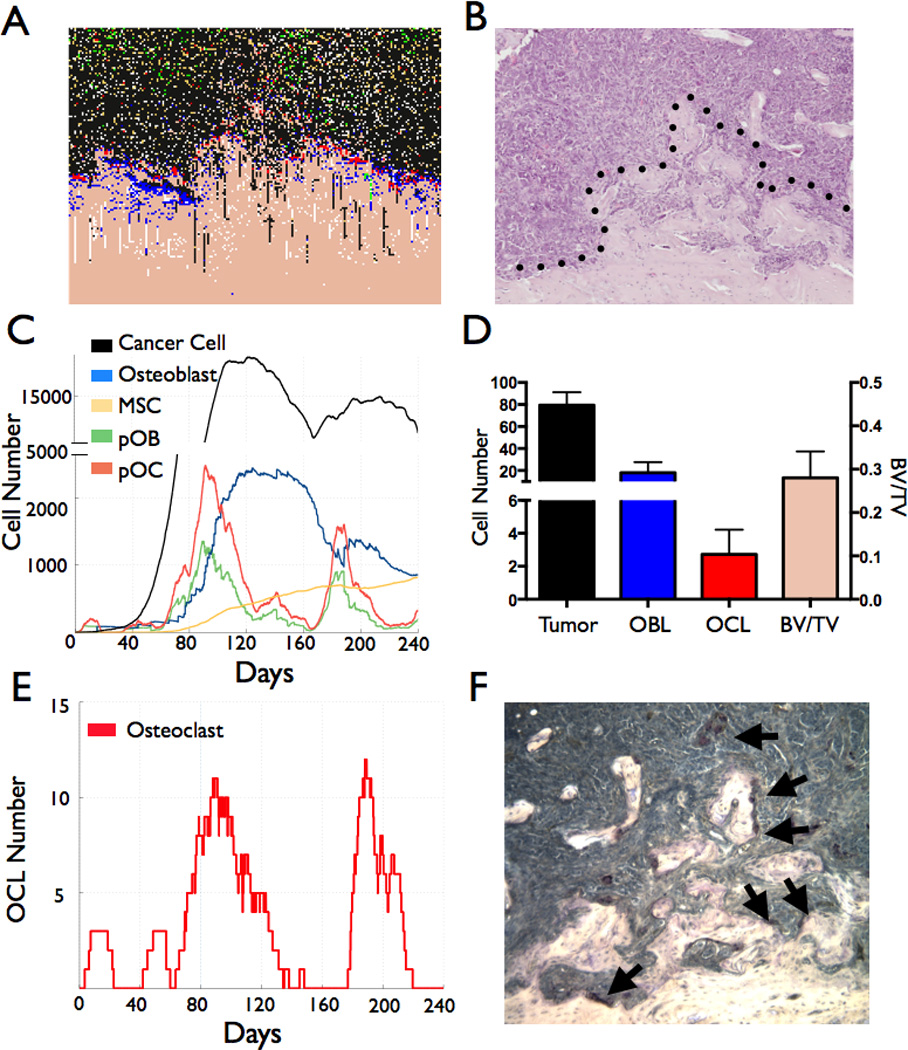
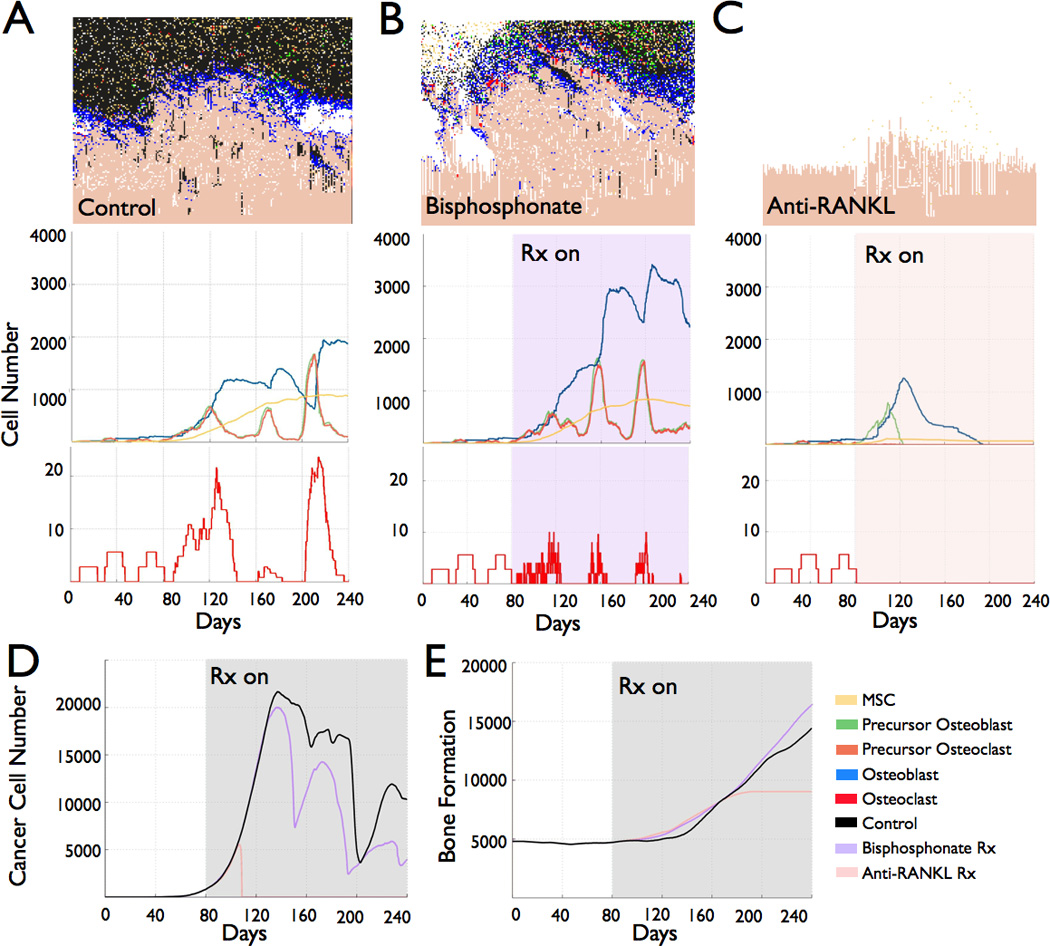
Bone metastasis will impact most men with advanced prostate cancer. The vicious cycle of bone degradation and formation driven by metastatic prostate cells in bone yields factors that drive cancer growth. Mechanistic insights into this vicious cycle have suggested new therapeutic opportunities, but complex temporal and cellular interactions in the bone microenvironment make drug development challenging. We have integrated biologic and computational approaches to generate a hybrid cellular automata model of normal bone matrix homeostasis and the prostate cancer-bone microenvironment. The model accurately reproduces the basic multicellular unit bone coupling process, such that introduction of a single prostate cancer cell yields a vicious cycle similar in cellular composition and pathophysiology to models of prostate-to-bone metastasis. Notably, the model revealed distinct phases of osteolytic and osteogenic activity, a critical role for mesenchymal stromal cells in osteogenesis, and temporal changes in cellular composition. To evaluate the robustness of the model, we assessed the effect of established bisphosphonate and anti-RANKL therapies on bone metastases. At approximately 100% efficacy, bisphosphonates inhibited cancer progression while, in contrast with clinical observations in humans, anti-RANKL therapy fully eradicated metastases. Reducing anti-RANKL yielded clinically similar results, suggesting that better targeting or dosing could improve patient survival. Our work establishes a computational model that can be tailored for rapid assessment of experimental therapies and delivery of precision medicine to patients with prostate cancer with bone metastases.
©2014 AACR.
Conflict of interest statement
Figures
References
-
- Keller ET, Brown J. Prostate cancer bone metastases promote both osteolytic and osteoblastic activity. J Cell Biochem. 2004;91:718–729. - PubMed
-
- Brown JE, Coleman RE. Denosumab in patients with cancer-a surgical strike against the osteoclast. Nature reviews Clinical oncology. 2012;9:110–118. - PubMed
-
- Bilezikian J, Raisz L, Martin T. Principles of Bone Biology. Academic Press; 2008.
-
- Bussard KM, Gay CV, Mastro AM. The bone microenvironment in metastasis; what is special about bone? Cancer Metastasis Rev. 2008;27:41–55. - PubMed
-
- Lynch CC. Matrix metalloproteinases as master regulators of the vicious cycle of bone metastasis. Bone. 2010 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
