

Effects of Patient Empowerment Programme (PEP) on clinical outcomes and health service utilization in type 2 diabetes mellitus in primary care: an observational matched cohort study
- PMID: 24788804
- PMCID: PMC4006782
- DOI: 10.1371/journal.pone.0095328
Effects of Patient Empowerment Programme (PEP) on clinical outcomes and health service utilization in type 2 diabetes mellitus in primary care: an observational matched cohort study
Abstract
Background: To evaluate the effects of a large population-based patient empowerment programme (PEP) on clinical outcomes and health service utilization rates in type 2 diabetes mellitus (T2DM) patients in the primary care setting.
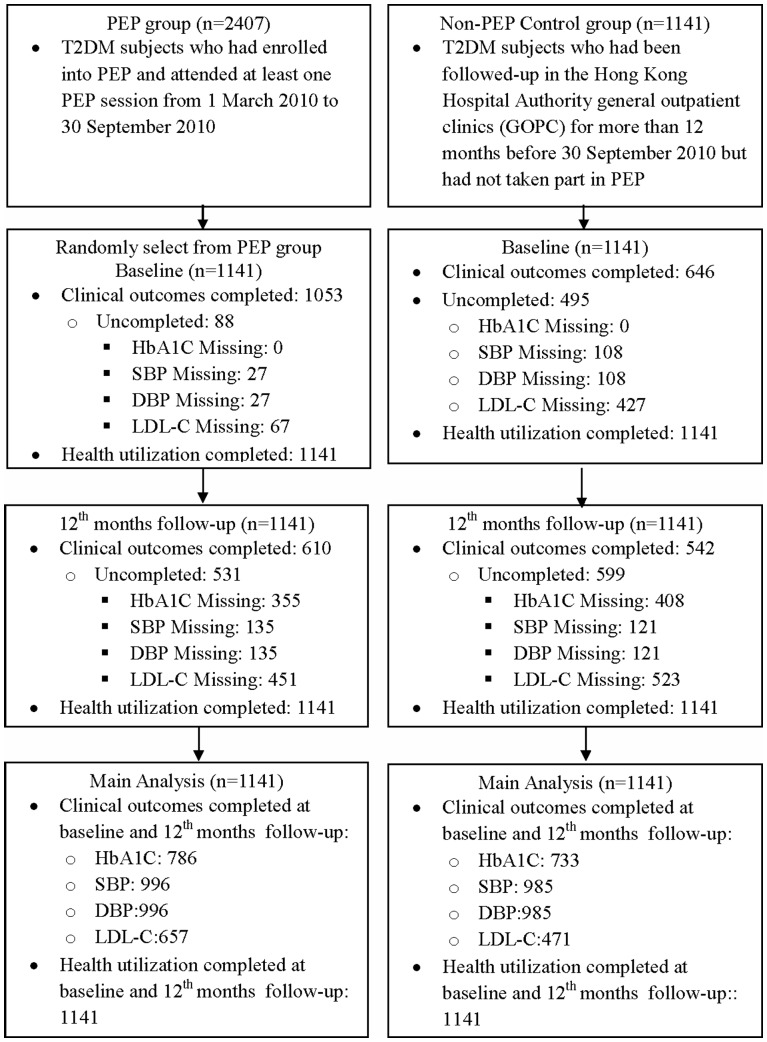
Research design and subjects: A stratified random sample of 1,141 patients with T2DM enrolled to PEP between March and September 2010 were selected from general outpatient clinics (GOPC) across Hong Kong and compared with an equal number of T2DM patients who had not participated in the PEP (non-PEP group) matched by age, sex and HbA1C level group.
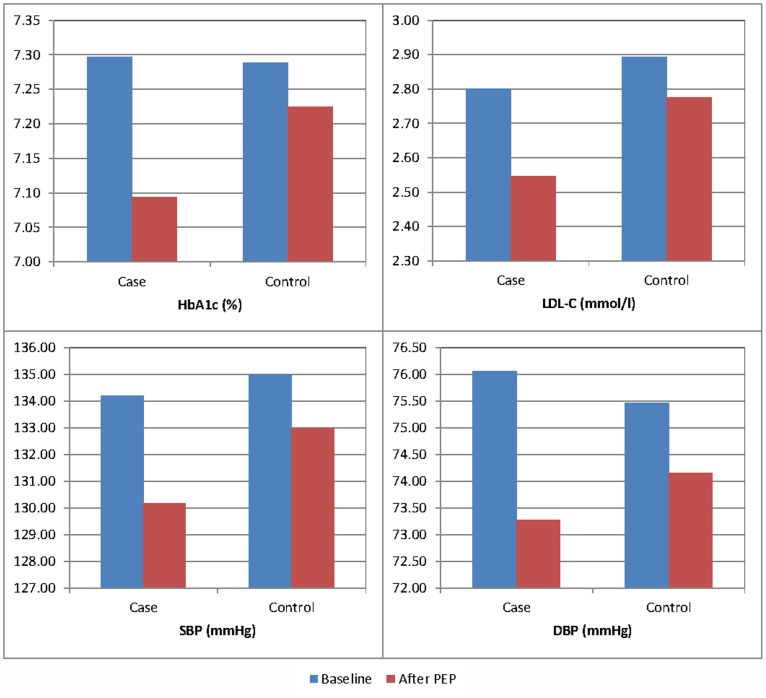
Measures: Clinical outcomes of HbA1c, SBP, DBP and LDL-C levels, and health service utilization rates including numbers of visits to GOPC, specialist outpatient clinics (SOPC), emergency department (ED) and inpatient admissions, were measured at baseline and at 12-month post-recruitment. The effects of PEP on clinical outcomes and health service utilization rates were assessed by the difference-in-difference estimation, using the generalized estimating equation models.
Results: Compared with non-PEP group, PEP group achieved additional improvements in clinical outcomes over the 12-month period. A significantly greater percentage of patients in the PEP group attained HbA1C≤7% or LDL-C≤2.6 mmol/L at 12-month follow-up compared with the non-PEP group. PEP group had a mean 0.813 fewer GOPC visits in comparison with the non-PEP group.
Conclusions: PEP was effective in improving the clinical outcomes and reduced the general outpatient clinic utilization rate over a 12-month period. Empowering T2DM patients on self-management of their disease can enhance the quality of diabetes care in primary care.
Trial registration: ClinicalTrials.gov NCT01935349.
Conflict of interest statement
Figures
References
-
- Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, et al. (2009) Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes care 32: 193–203. - PMC - PubMed
-
- Cheung BM, Ong KL, Cherny SS, Sham PC, Tso AW, et al. (2009) Diabetes prevalence and therapeutic target achievement in the United States, 1999 to 2006. The American journal of medicine 122: 443–453. - PubMed
-
- Wong KW, Ho SY, Chao DV (2012) Quality of diabetes care in public primary care clinics in Hong Kong. Family Practice 29: 196–202. - PubMed
-
- Funnell MM (2006) The Diabetes Attitudes, Wishes, and Needs (DAWN) Study. Clinical Diabetes 24: 154–155.
-
- Nutbeam D (1998) Health promotion glossary. Health Promotion International 13: 349–364.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
