

Accommodative intraocular lens versus standard monofocal intraocular lens implantation in cataract surgery
- PMID: 24788900
- PMCID: PMC10505746
- DOI: 10.1002/14651858.CD009667.pub2
Accommodative intraocular lens versus standard monofocal intraocular lens implantation in cataract surgery
Abstract
Background: Following cataract surgery and intraocular lens (IOL) implantation, loss of accommodation or postoperative presbyopia occurs and remains a challenge. Standard monofocal IOLs correct only distance vision; patients require spectacles for near vision. Accommodative IOLs have been designed to overcome loss of accommodation after cataract surgery.
Objectives: To define (a) the extent to which accommodative IOLs improve unaided near visual function, in comparison with monofocal IOLs; (b) the extent of compromise to unaided distance visual acuity; c) whether a higher rate of additional complications is associated the use of accommodative IOLs.
Search methods: We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2013, Issue 9), Ovid MEDLINE, Ovid MEDLINE in-Process and Other Non-Indexed Citations, Ovid MEDLINE Daily Update, Ovid OLDMEDLINE (January 1946 to October 2013), EMBASE (January 1980 to October 2013), Latin American and Caribbean Health Sciences Literature Database (LILACS) (January 1982 to October 2013), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrial.gov) and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not use any date or language restrictions in the electronic searches for trials. We last searched the electronic databases on 10 October 2013.
Selection criteria: We include randomised controlled trials (RCTs) which compared implantation of accommodative IOLs to implantation of monofocal IOLs in cataract surgery.
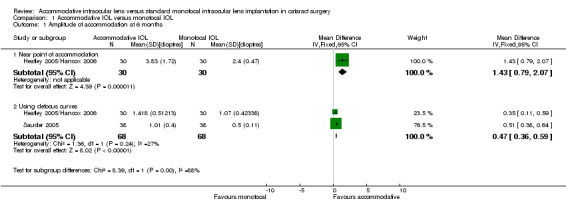
Data collection and analysis: Two authors independently screened search results, assessed risk of bias and extracted data. All included trials used the 1CU accommodative IOL (HumanOptics, Erlangen, Germany) for their intervention group. One trial had an additional arm with the AT-45 Crystalens accommodative IOL (Eyeonics Vision). We performed a separate analysis comparing 1CU and AT-45 IOL.
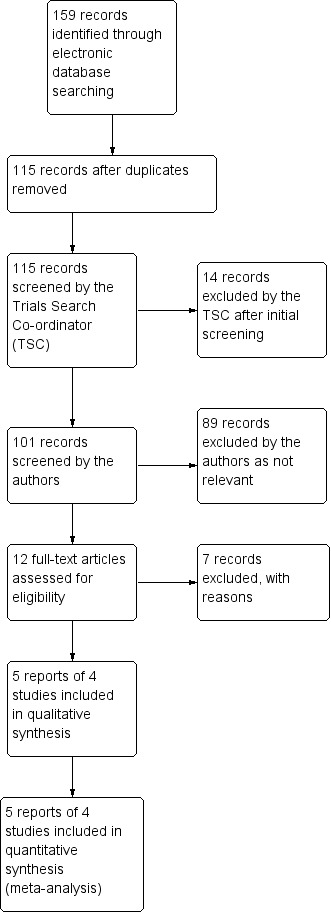
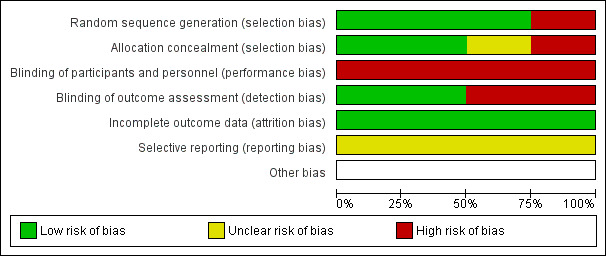
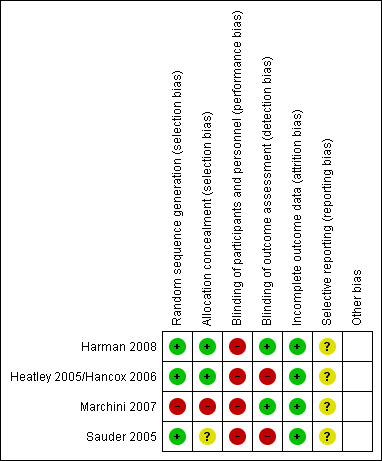
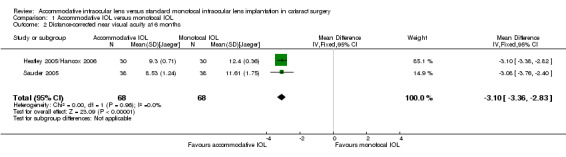
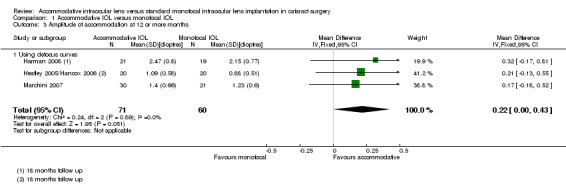
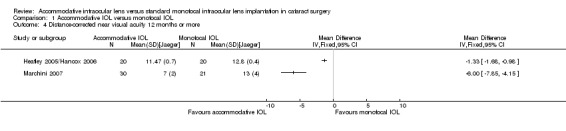
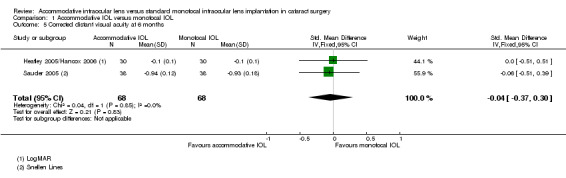
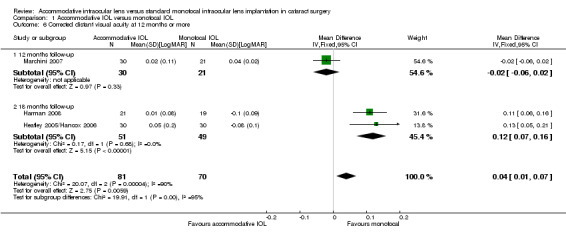
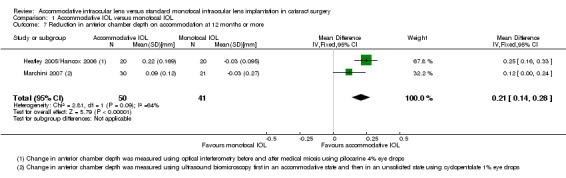
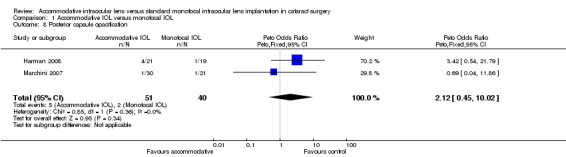
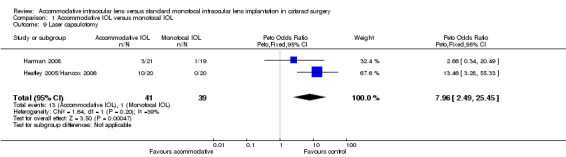
Main results: We included four RCTs, including 229 participants (256 eyes), conducted in Germany, Italy and the UK. The age range of participants was 21 to 87 years. All studies included people who had bilateral cataracts with no pre-existing ocular pathologies. We judged all studies to be at high risk of performance bias. We graded two studies with high risk of detection bias and one study with high risk of selection bias.Participants who received the accommodative IOLs achieved better distance-corrected near visual acuity (DCNVA) at six months (mean difference (MD) -3.10 Jaeger units; 95% confidence intervals (CI) -3.36 to -2.83, 2 studies, 106 people, 136 eyes, moderate quality evidence). Better DCNVA was seen in the accommodative lens group at 12 to 18 months in the three trials that reported this time point but considerable heterogeneity of effect was seen, ranging from 1.3 (95% CI 0.98 to 1.68; 20 people, 40 eyes) to 6 (95% CI 4.15 to 7.85; 51 people, 51 eyes) Jaeger units and 0.12 (95% CI 0.05 to 0.19; 40 people, binocular) logMAR improvement (low quality evidence). The relative effect of the lenses on corrected distant visual acuity (CDVA) was less certain. At six months there was a standardised mean difference of -0.04 standard deviations (95% CI -0.37 to 0.30, 2 studies, 106 people, 136 eyes, low quality evidence). At long-term follow-up there was heterogeneity of effect with 18-month data in two studies showing that CDVA was better in the monofocal group (MD 0.12 logMAR; 95% CI 0.07 to 0.16, 2 studies, 70 people,100 eyes) and one study which reported data at 12 months finding similar CDVA in the two groups (-0.02 logMAR units, 95% CI -0.06 to 0.02, 51 people) (low quality evidence).The relative effect of the lenses on reading speed and spectacle independence was uncertain, The average reading speed was 11.6 words per minute more in the accommodative lens group but the 95% confidence intervals ranged from 12.2 words less to 35.4 words more (1 study, 40 people, low quality evidence). People with accommodative lenses were more likely to be spectacle-independent but the estimate was very uncertain (risk ratio (RR) 8.18; 95% CI 0.47 to 142.62, 1 study, 40 people, very low quality evidence).More cases of posterior capsule opacification (PCO) were seen in accommodative lenses but the effect of the lenses on PCO was uncertain (Peto odds ratio (OR) 2.12; 95% CI 0.45 to 10.02, 91 people, 2 studies, low quality evidence). People in the accommodative lens group were more likely to require laser capsulotomy (Peto OR 7.96; 95% CI 2.49 to 25.45, 2 studies, 60 people, 80 eyes, low quality evidence). Glare was reported less frequently with accommodative lenses but the relative effect of the lenses on glare was uncertain (RR any glare 0.78; 95% CI 0.32 to 1.90, 1 study, 40 people, and RR moderate/severe glare 0.45; 95% CI 0.04 to 4.60, low quality evidence).
Authors' conclusions: There is moderate-quality evidence that study participants who received accommodative IOLs had a small gain in near visual acuity after six months. There is some evidence that distance visual acuity with accommodative lenses may be worse after 12 months but due to low quality of evidence and heterogeneity of effect, the evidence for this is not clear-cut. People receiving accommodative lenses had more PCO which may be associated with poorer distance vision. However, the effect of the lenses on PCO was uncertain.Further research is required to improve the understanding of how accommodative IOLs may affect near visual function, and whether they provide any durable gains. Additional trials, with longer follow-up, comparing different accommodative IOLs, multifocal IOLs and monofocal IOLs, would help map out their relative efficacy, and associated late complications. Research is needed on control over capsular fibrosis postimplantation.Risks of bias, heterogeneity of outcome measures and study designs used, and the dominance of one design of accommodative lens in existing trials (the HumanOptics 1CU) mean that these results should be interpreted with caution. They may not be applicable to other accommodative IOL designs.
Conflict of interest statement
None known.
Figures
Update of
- doi: 10.1002/14651858.CD009667
Similar articles
-
Multifocal versus monofocal intraocular lenses after cataract extraction.Cochrane Database Syst Rev. 2016 Dec 12;12(12):CD003169. doi: 10.1002/14651858.CD003169.pub4. Cochrane Database Syst Rev. 2016. PMID: 27943250 Free PMC article.
-
Intraocular lens optic edge design for the prevention of posterior capsule opacification after cataract surgery.Cochrane Database Syst Rev. 2021 Aug 16;8(8):CD012516. doi: 10.1002/14651858.CD012516.pub2. Cochrane Database Syst Rev. 2021. PMID: 34398965 Free PMC article.
-
Trifocal intraocular lenses versus bifocal intraocular lenses after cataract extraction among participants with presbyopia.Cochrane Database Syst Rev. 2023 Jan 27;1(1):CD012648. doi: 10.1002/14651858.CD012648.pub3. Cochrane Database Syst Rev. 2023. PMID: 36705482 Free PMC article.
-
Types of intraocular lenses for cataract surgery in eyes with uveitis.Cochrane Database Syst Rev. 2014 Mar 4;3(3):CD007284. doi: 10.1002/14651858.CD007284.pub2. Cochrane Database Syst Rev. 2014. PMID: 24590672 Free PMC article.
-
Trifocal versus extended depth of focus (EDOF) intraocular lenses after cataract extraction.Cochrane Database Syst Rev. 2024 Jul 10;7(7):CD014891. doi: 10.1002/14651858.CD014891.pub2. Cochrane Database Syst Rev. 2024. PMID: 38984608 Free PMC article.
Cited by
-
Clinical outcomes following trifocal diffractive intraocular lens implantation for age-related cataract in China.Clin Ophthalmol. 2018 Jul 26;12:1317-1324. doi: 10.2147/OPTH.S169215. eCollection 2018. Clin Ophthalmol. 2018. PMID: 30100704 Free PMC article.
-
Comparison of the Clinical Performance of Refractive Rotationally Asymmetric Multifocal IOLs with Other Types of IOLs: A Meta-Analysis.J Ophthalmol. 2018 Sep 27;2018:4728258. doi: 10.1155/2018/4728258. eCollection 2018. J Ophthalmol. 2018. PMID: 30363767 Free PMC article. Review.
-
Long-Term Clinical Outcomes after Mix and Match Implantation of Two Multifocal Intraocular Lenses with Different Adds.J Ophthalmol. 2019 Jan 14;2019:6789263. doi: 10.1155/2019/6789263. eCollection 2019. J Ophthalmol. 2019. PMID: 30755802 Free PMC article.
-
Accommodative intraocular lenses: where are we and where we are going.Eye Vis (Lond). 2017 Jun 26;4:16. doi: 10.1186/s40662-017-0077-7. eCollection 2017. Eye Vis (Lond). 2017. PMID: 28674696 Free PMC article. Review.
-
Altered stress field of the human lens capsule after cataract surgery.J Biomech. 2021 Jan 22;115:110127. doi: 10.1016/j.jbiomech.2020.110127. Epub 2020 Nov 10. J Biomech. 2021. PMID: 33223144 Free PMC article.
References
References to studies included in this review
Harman 2008 {published data only}
-
- Harman FE, Maling S, Kampougeris G, Langan L, Khan I, Lee N, et al. Comparing the 1CU accommodative, multifocal, and monofocal intraocular lenses: a randomized trial. Ophthalmology 2008;115(6):993‐1001. - PubMed
Heatley 2005/Hancox 2006 {published data only}
-
- Hancox J, Spalton D, Heatley C, Jayaram H, Marshall J. Objective measurement of intraocular lens movement and dioptric change with a focus shift accommodating intraocular lens. Journal of Cataract and Refractive Surgery 2006;32(7):1098‐1103. - PubMed
-
- Heatley CJ, Spalton DJ, Hancox J, Kumar A, Marshall J. Fellow eye comparison between the 1CU accommodative intraocular lens and the Acrysof MA30 monofocal intraocular lens. American Journal of Ophthalmology 2005;140(2):207‐13. - PubMed
Marchini 2007 {published data only}
-
- Marchini G, Mora P, Pedrotti E, Manzotti F, Aldigeri R, Gandolfi SA. Functional assessment of two different accommodative intraocular lenses compared with a monofocal intraocular lens. Ophthalmology 2007;114(11):2038‐43. - PubMed
References to studies excluded from this review
Beiko 2013 {published data only}
-
- Beiko GH. Comparison of visual results with accommodating intraocular lenses versus mini‐monovision with a monofocal intraocular lens. Journal of Cataract and Refractive Surgery 2013;39(1):48‐55. - PubMed
Findl 2004 {published data only}
-
- Findl O, Kriechbaum K, Menapace R, Koeppl C, Sacu S, Wirtitsch M, et al. Laserinterferometric assessment of pilocarpine‐induced movement of an accommodating intraocular lens: a randomized trial. Ophthalmology 2004;111(8):1515‐21. - PubMed
Kamppeter 2005 {published data only}
-
- Kamppeter BA, Sauder G, Jonas JB. Contrast and glare sensitivity after implantation of AcrySof and Human Optics 1CU intraocular lenses. European Journal of Ophthalmology 2005;15(4):458‐61. - PubMed
Mesci 2010 {published data only}
-
- Mesci C, Erbil H, Ozdoker L, Karakurt Y, Bilge AD. Visual acuity and contrast sensitivity function after accommodative and multifocal intraocular lens implantation. European Journal of Ophthalmology 2010;20(1):90‐100. - PubMed
Wang 2005 {published data only}
-
- Wang CY, Ma B, Wang LL. Clinical accommodative status study of the accommodative foldable intraocular lens. International Journal of Ophthalmology 2005;5(4):669‐71.
Wolffsohn 2006 {published data only}
Xu 2007 {published data only}
-
- Xu M, Li WS, Zhao YE, Wang QM. The clinical efficacy of accommodative intraocular lens and multifocal intraocular lens in pseudophakic after phacoemulsification. Chinese Journal of Ophthalmology 2007;43(2):104‐7. - PubMed
Additional references
Alió 2006
-
- Alió JL, Chaubard JJ, Caliz A, Sala E, Patel S. Correction of presbyopia by technovision central multifocal LASIK (presbyLASIK). Journal of Refractive Surgery 2006;22(5):453‐60. - PubMed
Avitabile 2001
-
- Avitabile T, Marano F. Multifocal intra‐ocular lenses. Current Opinion in Ophthalmology 2001;12(1):12‐6. - PubMed
Boerner 1984
-
- Boerner CF, Thrasher BH. Results of monovision correction in bilateral pseuophakes. American Intraocular Implant Society Journal 1984;10:49‐51. - PubMed
Chandhrasi 2006
-
- Chandhrasi S, Knorz MC. Comparison of higher order aberrations and contrast sensitivity after LASIK, Verisyse phakic IOL, and Array multifocal IOL. Journal of Refractive Surgery 2006;22(3):231‐6. - PubMed
CONSORT 2012
-
- Altman DG, Moher D, Schultz KF. Improving the reporting of randomised trials: The CONSORT statement and beyond. Statistics in Medicine 2012;31(25):2985‐97. - PubMed
Croft 2001
-
- Croft MA, Glasser A, Kaufman PL. Accommodation and presbyopia. International Ophthalmology Clinics 2001;41(2):33‐46. - PubMed
Datiles 1990
-
- Datiles MB, Gancayco T. Low myopia with low astigmatic correction gives cataract surgery patients good depth of focus. Ophthalmology 1990;97(7):922‐6. - PubMed
Deeks 2011
-
- Deeks JJ, Higgins JPT, Altman DG (editors). Chapter 9: Analysing data and undertaking meta‐analyses In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Findl 2007
-
- Findl O, Leydolt C. Meta‐analysis of accommodating intraocular lenses. Journal of Cataract and Refractive Surgery 2007;33(3):522‐7. - PubMed
Glanville 2006
Glasser 1999
-
- Glasser A, Campbell MC. Biometric, optical and physical changes in the isolated human crystalline lens with age in relation to presbyopia. Vision Research 1999;39(11):1991‐2015. - PubMed
Greenbaum 2002
-
- Greenbaum S. Monovision pseudophakia. Journal of Cataract and Refractive Surgery 2002;28(8):1439‐43. - PubMed
Higgins 2003
Higgins 2011
-
- Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Javitt 2000
-
- Javitt JC, Steinert RF. Cataract extraction with multifocal intraocular lens implantation: a multinational clinical trial evaluating clinical, functional and quality of life outcomes. Ophthalmology 2000;107(11):2040‐8. - PubMed
Keates 1995
-
- Keates RH, Martines E, Tennen DG, Reich C. Small‐diameter corneal inlay in presbyopic or pseudophakic patients. Journal of Cataract and Refractive Surgery 1995;21(5):519‐21. - PubMed
Küchle 2004
-
- Küchle M, Seitz B, Langenbucher A, Gusek‐Schneider GC, Martus P, Nguyen NX, et al. Comparison of 6‐month results of implantation of the 1CU accommodative intraocular lens with conventional intraocular lenses. Ophthalmology 2004;111(2):318‐24. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Leyland 2003
-
- Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery; a systematic review. Ophthalmology 2003;110(9):1789‐98. - PubMed
Mathews 1999
-
- Mathews S. Scleral expansion surgery does not restore accommodation in human presbyopia. Ophthalmology 1999;106(5):873‐7. - PubMed
Menapace 2007
-
- Menapace R, Findl O, Kriechbaum K, Leydolt‐Koeppl Ch. Accommodating intraocular lenses: a critical review of present and future concepts. Graefe's Archive for Clinical and Experimental Ophthalmology 2007;245(4):473‐89. - PubMed
Nijkamp 2004
-
- Nijkamp MD, Dolders MG, Brabander J, Borne B, Hendrikse F, Nuijts RM. Effectiveness of multifocal intraocular lenses to correct presbyopia after cataract surgery; a randomized controlled trial. Ophthalmology 2004;111(10):1832‐9. - PubMed
Pineda‐Fernandez 2004
-
- Pineda‐Fernandez A, Jaramillo J, Celis V, Vargas J, DiStacio M, Galindez A, et al. Refractive outcomes after bilateral multifocal intraocular lens implantation. Journal of Cataract and Refractive Surgery 2004;30(3):685‐8. - PubMed
Review Manager 2012 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Uthoff 2007
-
- Uthoff D, Gulati A, Hepper D, Holland D. Potentially accommodating 1CU intraocular lens: 1‐year results in 553 eyes and literature review. Journal of Refractive Surgery 2007;23(2):159‐71. - PubMed
WHO 2011
-
- World Health Organization. Prevention of blindness and visual impairment: priority eye diseases. www.who.int/blindness/causes/priority/en/index1.html (accessed 5 October 2011).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials