

Mixed Mycobacterium tuberculosis complex infections and false-negative results for rifampin resistance by GeneXpert MTB/RIF are associated with poor clinical outcomes
- PMID: 24789181
- PMCID: PMC4097703
- DOI: 10.1128/JCM.02489-13
Mixed Mycobacterium tuberculosis complex infections and false-negative results for rifampin resistance by GeneXpert MTB/RIF are associated with poor clinical outcomes
Abstract
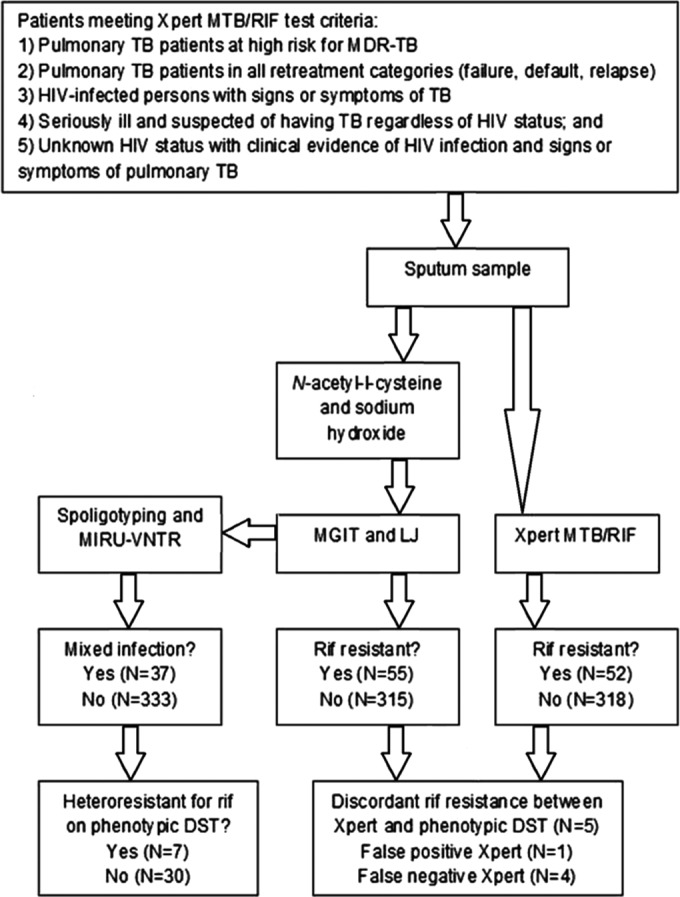
The Xpert MTB/RIF (Xpert) assay is becoming a principal screening tool for diagnosing rifampin-resistant Mycobacterium tuberculosis complex (MTBC) infection. However, little is known about the performance of the Xpert assay in infections with both drug-sensitive and drug-resistant strains (mixed MTBC infections). We assessed the performance of the Xpert assay for detecting rifampin resistance using phenotypic drug sensitivity testing (DST) as the reference standard in 370 patients with microbiologically proven pulmonary tuberculosis. Mixed MTBC infections were identified genetically through 24-locus mycobacterial interspersed repetitive-unit-variable-number tandem-repeat (MIRU-VNTR) analysis. Logistic regression was used to identify the factors associated with poor (defined as treatment failure, default, and death from any cause) or good (defined as cure or successful treatment completion) clinical outcomes. The analytic sensitivity of the Xpert assay for detecting rifampin resistance was assessed in vitro by testing cultures containing different ratios of drug-sensitive and drug-resistant organisms. Rifampin resistance was detected by the Xpert assay in 52 (14.1%) and by phenotypic DST in 55 (14.9%) patients. Mixed MTBC infections were identified in 37 (10.0%) patients. The Xpert assay was 92.7% (95% confidence interval [CI], 82.4% to 97.9%) sensitive for detecting rifampin resistance and 99.7% (95% CI, 98.3% to 99.9%) specific. When restricted to patients with mixed MTBC infections, Xpert sensitivity was 80.0% (95% CI, 56.3 to 94.3%). False-negative Xpert results (adjusted odds ratio [aOR], 6.6; 95% CI,1.2 to 48.2) and mixed MTBC infections (aOR, 6.5; 95% CI, 2.1 to 20.5) were strongly associated with poor clinical outcome. The Xpert assay failed to detect rifampin resistance in vitro when <90% of the organisms in the sample were rifampin resistant. Our study indicates that the Xpert assay has an increased false-negative rate for detecting rifampin resistance with mixed MTBC infections. In hyperendemic settings where mixed infections are common, the Xpert results might need further confirmation.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Zumla A, Abubakar I, Raviglione M, Hoelscher M, Ditiu L, McHugh TD, Squire SB, Cox H, Ford N, McNerney R, Marais B, Grobusch M, Lawn SD, Migliori GB, Mwaba P, O'Grady J, Pletschette M, Ramsay A, Chakaya J, Schito M, Swaminathan S, Memish Z, Maeurer M, Atun R. 2012. Drug-resistant tuberculosis–current dilemmas, unanswered questions, challenges, and priority needs. J. Infect. Dis. 205(Suppl 2):S228–S240. 10.1093/infdis/jir858 - DOI - PubMed
-
- Falzon D, Jaramillo E, Schünemann HJ, Arentz M, Bauer M, Bayona J, Blanc L, Caminero JA, Daley CL, Duncombe C, Fitzpatrick C, Gebhard A, Getahun H, Henkens M, Holtz TH, Keravec J, Keshavjee S, Khan AJ, Kulier R, Leimane V, Lienhardt C, Lu C, Mariandyshev A, Migliori GB, Mirzayev F, Mitnick CD, Nunn P, Nwagboniwe G, Oxlade O, Palmero D, Pavlinac P, Quelapio MI, Raviglione MC, Rich ML, Royce S, Rüsch-Gerdes S, Salakaia A, Sarin R, Sculier D, Varaine F, Vitoria M, Walson JL, Wares F, Weyer K, White RA, Zignol M. 2011. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur. Respir. J. 38:516–528. 10.1183/09031936.00073611 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
