

A systematic review of transarterial embolization versus emergency surgery in treatment of major nonvariceal upper gastrointestinal bleeding
- PMID: 24790465
- PMCID: PMC3998850
- DOI: 10.2147/CEG.S56725
A systematic review of transarterial embolization versus emergency surgery in treatment of major nonvariceal upper gastrointestinal bleeding
Abstract
Background: Emergency surgery or transarterial embolization (TAE) are options for the treatment of recurrent or refractory nonvariceal upper gastrointestinal bleeding. Surgery has the disadvantage of high rates of postoperative morbidity and mortality. Embolization has become more available and has the advantage of avoiding laparotomy in this often unfit and elderly population.
Objective: To carry out a systematic review and meta-analysis of all studies that have directly compared TAE with emergency surgery in the treatment of major upper gastrointestinal bleeding that has failed therapeutic upper gastrointestinal endoscopy.
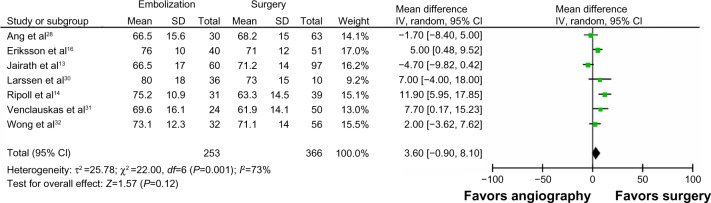
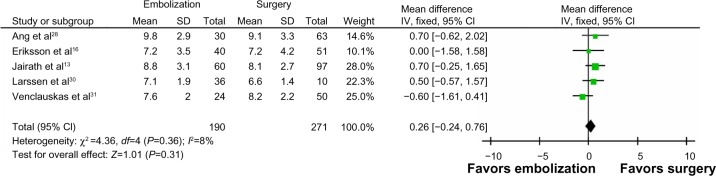
Methods: A literature search of Ovid MEDLINE, Embase, and Google Scholar was performed. The primary outcomes were all-cause mortality and rates of rebleeding. The secondary outcomes were length of stay and postoperative complications.
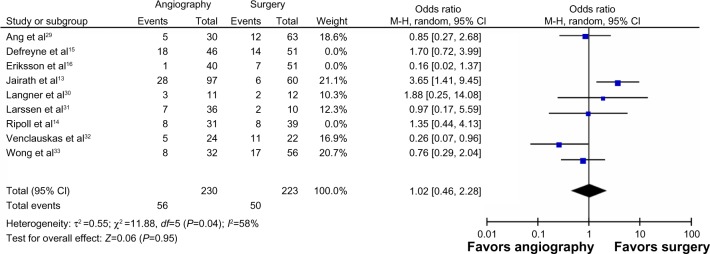
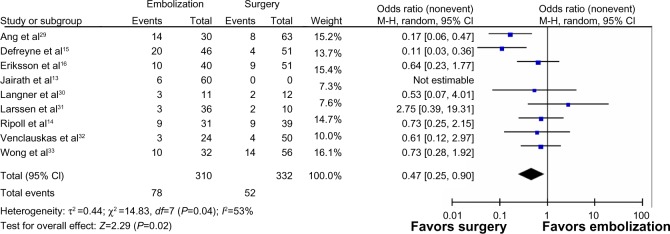
Results: A total of nine studies with 711 patients (347 who had embolization and 364 who had surgery) were analyzed. Patients in the TAE group were more likely to have ischemic heart disease (odds ratio [OR] =1.99; 95% confidence interval [CI]: 1.33, 2.98; P=0.0008; I (2)=67% [random effects model]) and be coagulopathic (pooled OR =2.23; 95% CI: 1.29, 3.87; P=0.004; I (2)=33% [fixed effects model]). Compared with TAE, surgery was associated with a lower risk of rebleeding (OR =0.41; 95% CI: 0.22, 0.77; P<0.0001; I (2)=55% [random effects]). There was no difference in mortality (OR =0.70; 95% CI: 0.48, 1.02; P=0.06; I (2)=44% [fixed effects]) between TAE and surgery.
Conclusion: When compared with surgery, TAE had a significant increased risk of rebleeding rates after TAE; however, there were no differences in mortality rates. These findings are subject to multiple sources of bias due to poor quality studies. These findings support the need for a well-designed clinical trial to ascertain which technique is superior.
Keywords: GI hemmorhage; interventional radiology; meta-analysis; radiology; surgery.
Figures
References
-
- Ang D, Teo EK, Tan A, et al. A comparison of surgery versus transcatheter angiographic embolization in the treatment of nonvariceal upper gastrointestinal bleeding uncontrolled by endoscopy. Eur J Gastroenterol Hepatol. 2012;24(8):929–938. - PubMed
-
- Defreyne L, De Schrijver I, Decruyenaere J, et al. Therapeutic decision-making in endoscopically unmanageable nonvariceal upper gastrointestinal hemorrhage. Cardiovasc Intervent Radiol. 2008;31(5):897–905. - PubMed
-
- Eriksson LG, Ljungdahl M, Sundbom M, Nyman R. Transcatheter arterial embolization versus surgery in the treatment of upper gastrointestinal bleeding after therapeutic endoscopy failure. J Vasc Interv Radiol. 2008;19(10):1413–1418. - PubMed
-
- Jairath V, Kahan BC, Logan RF, et al. National audit of the use of surgery and radiological embolization after failed endoscopic haemostasis for non-variceal upper gastrointestinal bleeding. Br J Surg. 2012;99(12):1672–1680. - PubMed
-
- Langner I, Langner S, Partecke LI, et al. Acute upper gastrointestinal hemorrhage: is a radiological interventional approach an alternative to emergency surgery? Emerg Radiol. 2008;15(6):413–419. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
