

Sustained CD4+ T cell-driven lymphopenia without a compensatory IL-7/IL-15 response among high-grade glioma patients treated with radiation and temozolomide
- PMID: 24790790
- PMCID: PMC4004618
- DOI: 10.4161/onci.27357
Sustained CD4+ T cell-driven lymphopenia without a compensatory IL-7/IL-15 response among high-grade glioma patients treated with radiation and temozolomide
Abstract
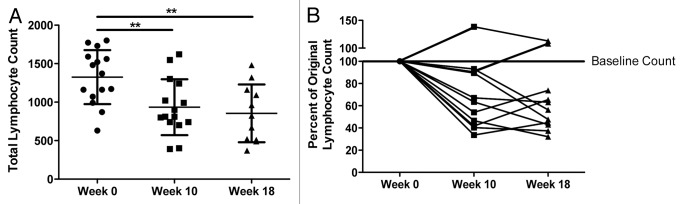
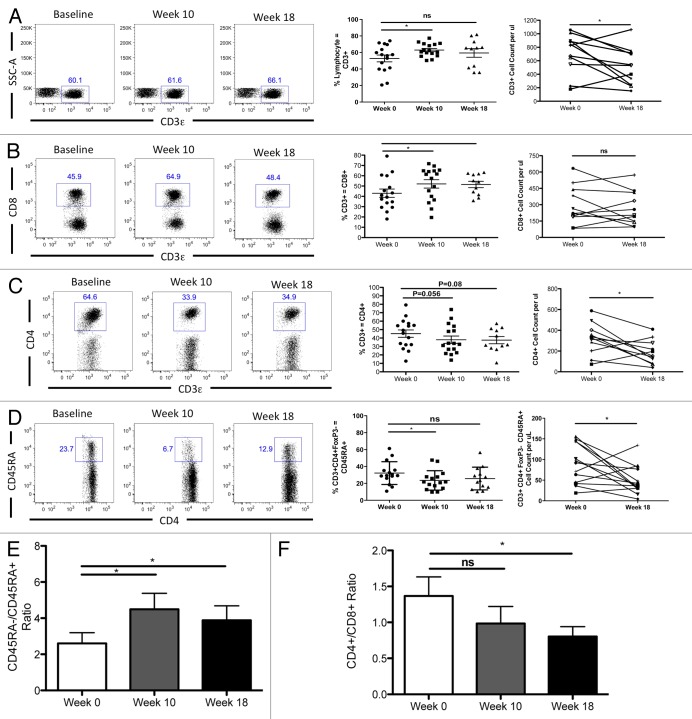
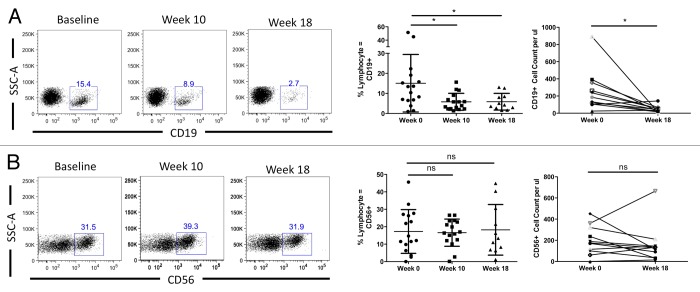
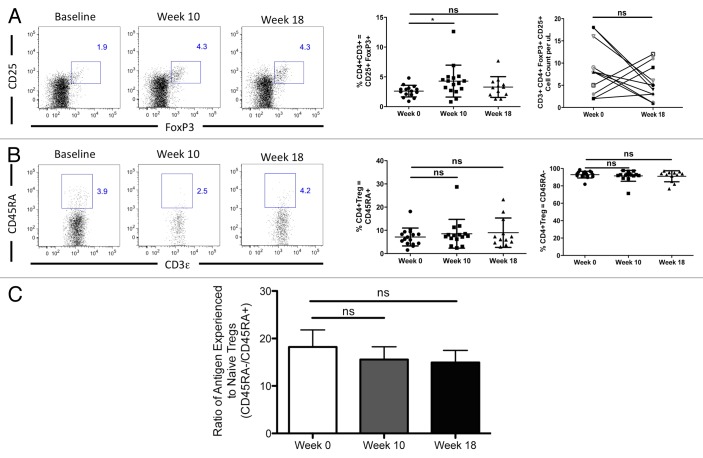
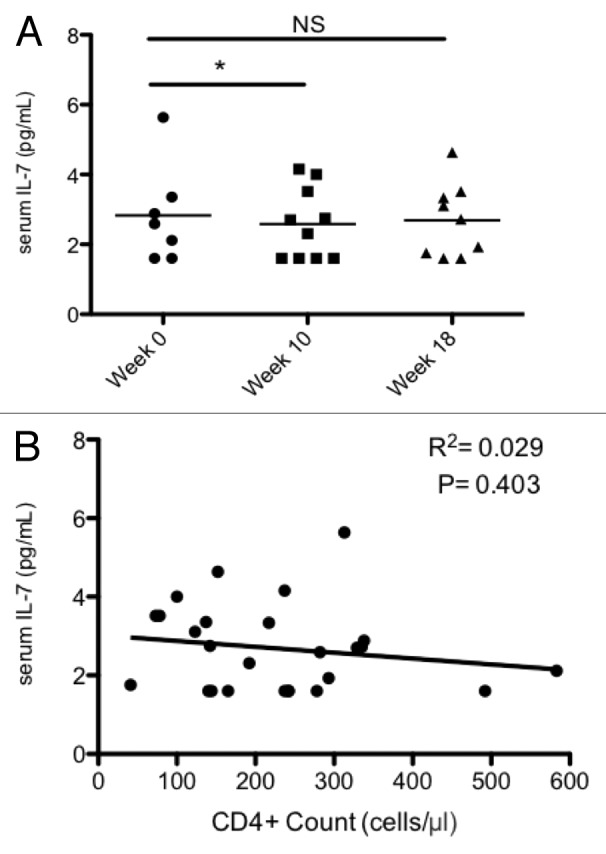
Prolonged lymphopenia correlating with decreased survival commonly occurs among glioma patients undergoing radiation therapy (RT) and temozolomide (TMZ) treatment. To better understand the pathophysiology of this phenomenon, we prospectively monitored serum cytokine levels and lymphocyte subsets in 15 high-grade glioma patients undergoing combined radiation and TMZ (referred to as RT/TMZ) treatment. Sufficient data for analysis were acquired from 11 of the patients initially enrolled. Lymphocyte phenotyping data were obtained using cytofluorometric analysis and serum cytokine levels were measured using the a multiplex bead-based assays. Total lymphocyte counts (TLCs) were > 1000 cells per μL peripheral blood in 10/11 patients at baseline, but dropped significantly after treatment. Specifically, after RT/TMZ therapy, the TLCs were found to be < 500 cells/μL in 2/11 patients, 500-1000 cells/μL in 7/11 patients, and > 1000 cells/μL in the remaining 2 patients. Among residual mononuclear blood cells, we observed a proportional drop in B and CD4+ T cells but not in CD8+ T lymphocytes. Natural killer cells remained to near-to-baseline levels and there was a transient and slight (insignificant) increase in regulatory T cells (Tregs). The circulating levels of IL-7 and IL-15 remained low despite marked drops in both the total and CD4+ T lymphocyte counts. Thus, patients with malignant glioma undergoing RT/TMZ treatment exhibit a marked decline in TLCs, affecting both CD4+ T cells and B lymphocytes, in the absence of a compensatory increase in interleukin-7 levels. The failure to mount an appropriate homeostatic cytokine response may be responsible for the prolonged lymphopenia frequently observed in these patients.
Keywords: CD4+ lymphopenia; IL-7; glioblastoma; immunotherapy; lymphocytes; radiation therapy; radiotherapy.
Figures
Similar articles
-
Serial changes in lymphocyte subsets in patients with newly diagnosed high grade astrocytomas treated with standard radiation and temozolomide.J Neurooncol. 2017 Nov;135(2):343-351. doi: 10.1007/s11060-017-2580-z. Epub 2017 Jul 29. J Neurooncol. 2017. PMID: 28756593
-
Pre-radiation lymphocyte harvesting and post-radiation reinfusion in patients with newly diagnosed high grade gliomas.J Neurooncol. 2015 Sep;124(2):307-16. doi: 10.1007/s11060-015-1841-y. Epub 2015 Jun 13. J Neurooncol. 2015. PMID: 26070554 Free PMC article.
-
Long-Acting Recombinant Human Interleukin-7, NT-I7, Increases Cytotoxic CD8 T Cells and Enhances Survival in Mouse Glioma Models.Clin Cancer Res. 2022 Mar 15;28(6):1229-1239. doi: 10.1158/1078-0432.CCR-21-0947. Clin Cancer Res. 2022. PMID: 35031547
-
Immune modulations during chemoimmunotherapy & novel vaccine strategies--in metastatic melanoma and non small-cell lung cancer.Dan Med J. 2013 Dec;60(12):B4774. Dan Med J. 2013. PMID: 24355457 Review.
-
The need for paradigm shift: prognostic significance and implications of standard therapy-related systemic immunosuppression in glioblastoma for immunotherapy and oncolytic virotherapy.Front Immunol. 2024 Feb 8;15:1326757. doi: 10.3389/fimmu.2024.1326757. eCollection 2024. Front Immunol. 2024. PMID: 38390330 Free PMC article. Review.
Cited by
-
Combining Radiation Therapy with Immune Checkpoint Blockade for Central Nervous System Malignancies.Front Oncol. 2016 Oct 7;6:212. doi: 10.3389/fonc.2016.00212. eCollection 2016. Front Oncol. 2016. PMID: 27774435 Free PMC article. Review.
-
Serum macrophage-derived chemokine/CCL22 levels are associated with glioma risk, CD4 T cell lymphopenia and survival time.Int J Cancer. 2015 Aug 15;137(4):826-36. doi: 10.1002/ijc.29441. Epub 2015 Feb 2. Int J Cancer. 2015. PMID: 25604093 Free PMC article.
-
Activation of 4-1BBL+ B cells with CD40 agonism and IFNγ elicits potent immunity against glioblastoma.J Exp Med. 2021 Jan 4;218(1):e20200913. doi: 10.1084/jem.20200913. J Exp Med. 2021. PMID: 32991668 Free PMC article.
-
The multidrug-resistance transporter Abcc3 protects NK cells from chemotherapy in a murine model of malignant glioma.Oncoimmunology. 2015 Oct 29;5(5):e1108513. doi: 10.1080/2162402X.2015.1108513. eCollection 2016 May. Oncoimmunology. 2015. PMID: 27467914 Free PMC article.
-
Field size effects on the risk and severity of treatment-induced lymphopenia in patients undergoing radiation therapy for solid tumors.Adv Radiat Oncol. 2018 Oct 23;3(4):512-519. doi: 10.1016/j.adro.2018.08.014. eCollection 2018 Oct-Dec. Adv Radiat Oncol. 2018. PMID: 30370350 Free PMC article. Review.
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, et al. European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups. National Cancer Institute of Canada Clinical Trials Group Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–66. doi: 10.1016/S1470-2045(09)70025-7. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials