

Techniques to define segmental anatomy during segmentectomy
- PMID: 24790841
- PMCID: PMC3988309
- DOI: 10.3978/j.issn.2225-319X.2014.02.03
Techniques to define segmental anatomy during segmentectomy
Abstract
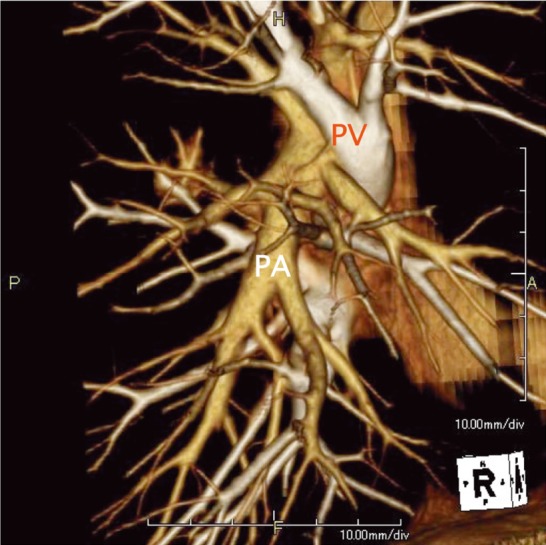
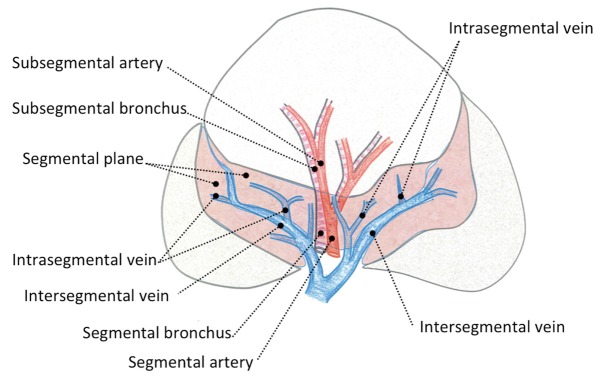
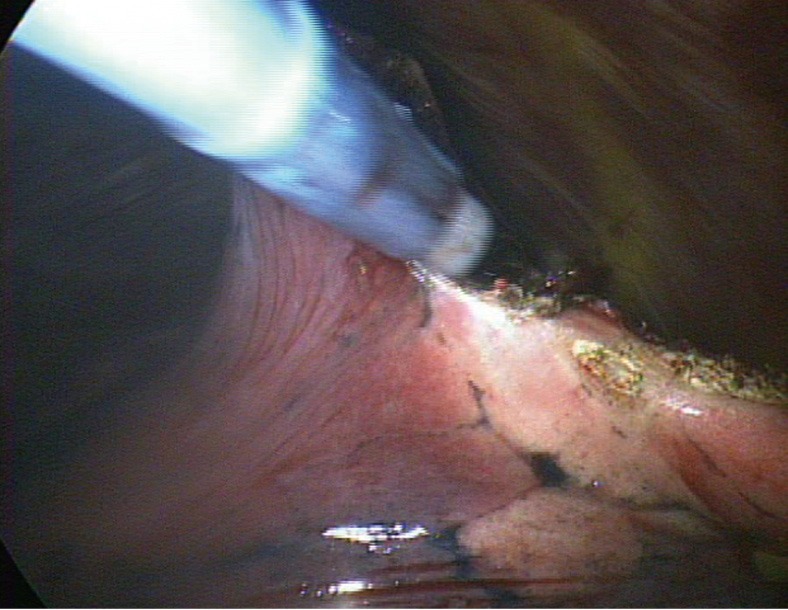
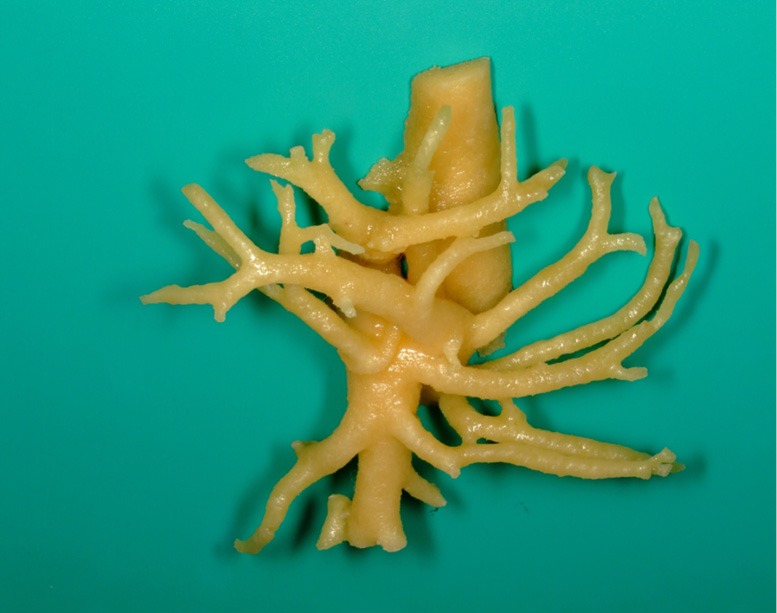
Pulmonary segmentectomy is generally acknowledged to be more technically complex than lobectomy. Three-dimensional computed tomography (3D CT) angiography is useful for understanding the pulmonary arterial and venous branching, as well as planning the surgery to secure adequate surgical margins. Comprehension of the intersegmental and intrasegmental veins makes the parenchymal dissection easier. To visualize the segmental border, creation of an inflation-deflation line by using a method of inflating the affected segment has become the standard in small-sized lung cancer surgery. Various modifications to create the segmental demarcation line have been devised to accurately perform the segmentectomy procedure.
Keywords: Segmentectomy; slip knot; subsegmentectomy; thoracoscopy; three-dimensional computed tomography (3D CT); video-assisted thoracic surgery (VATS).
Figures

References
-
- Yoshida J, Nagai K, Yokose T, et al. Limited resection trial for pulmonary ground-glass opacity nodules: fifty-case experience. J Thorac Cardiovasc Surg 2005;129:991-6 - PubMed
-
- Nakayama H, Yamada K, Saito H, et al. Sublobar resection for patients with peripheral small adenocarcinomas of the lung: surgical outcome is associated with features on computed tomographic imaging. Ann Thorac Surg 2007;84:1675-9 - PubMed
-
- Asamura H.Minimally invasive approach to early, peripheral adenocarcinoma with ground-glass opacity appearance. Ann Thorac Surg 2008;85:S701-4 - PubMed
-
- Schuchert MJ, Pettiford BL, Keeley S, et al. Anatomic segmentectomy in the treatment of stage I non-small cell lung cancer. Ann Thorac Surg 2007;84:926-32; discussion 932-3 - PubMed
-
- Boyden EA. A critique of the international nomenclature on bronchopulmonary segments. Dis Chest 1953;23:266-9 - PubMed
LinkOut - more resources
Full Text Sources