

doi: 10.4103/0972-2327.128693.
Surgery for drug-resistant focal epilepsy
Affiliations
- PMID: 24791080
- PMCID: PMC4001234
- DOI: 10.4103/0972-2327.128693
Item in Clipboard
Surgery for drug-resistant focal epilepsy
Ann Indian Acad Neurol.
2014 Mar.
Abstract
During the colloquium on drug-resistant epilepsy (DRE) at National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore on August 16-18, 2013, a number of presentations were made on the surgically remediable lesional epilepsy syndromes, presurgical evaluation, surgical techniques, neuropathology of drug resistance focal epilepsy and surgical outcome. This pictorial essay with the illustrative case examples provides an overview of the various surgical techniques for the management of drug-resistant focal epilepsy.
Keywords: Drug-resistant epilepsy; epilepsy; epilepsy surgery; surgical techniques.
Conflict of interest statement
Figures

(Case 1): (Panel a) shows high resolution T2 coronal images perpendicular to the hippocampus that reveals loss of volume of left hippocampus associated with loss of internal architecture. (Panel b) shows ictal EEG buildup of theta activity with sharp waves in the left temporal region. (Panel c) shows loss of neurons in CA1, Ca3, and CA4 on Neu N stains suggestive of mesial temporal sclerosis (hippocampal sclerosis) (NeunxObj.10), EEG = Electroencephalography

(Case 2): FLAIR coronal (panel a) and T2W (panel b) images showing atrophy and hyperintensity of both hippocampi suggestive of bilateral mesial temporal sclerosis and EEG features in the (panel c) FLAIR = Fluid attenuated inversion recovery, EEG = Electroencephalography

(a) (Case 3a): T2 axial brain FSE image (panel a) reveals focal cortical thickening and indistinct gray white junction of the right post central and angular gyrus. The fMRI overlaid on the T1 axial image (panel b) reveals that the left finger tapping induced BOLD activation of the motor cortex is located anterior to the dysplastic lesion. (Panel c) shows phase reversal at the right central (C4) in the ictal EEG. FSE = Fast spin echo, fMRI = functional magnetic resonance imaging, EEG = Electroencephalography

(b) (Case 3b): Focal cortical dysplasia type 2b (ILAE 2011): histology reveals complete dyslamination with large Taylor-type “balloon” neurons in dysplastic cortex (a) with enlarged soma, marginated Nissl substance (arrow), or glassy cytoplasm (block arrow) (b) that are labeled by GFAP (c). (A: H and E × Obj.10; B: H and E × obj.40; C: GFAP × Obj.40) ILAE = International League against Epilepsy, GFAP = Glial fibrillary acidic protein, H and E = Hematoxylin and eosin

(Case 4): FLAIR and T2 sagittal (panel a and b) images showing hyperintensity and atrophy of the involved right cerebral hemisphere suggestive of left insular and perisylvian gliosis FLAIR = Fluid attenuated inversion recovery

(a) (Case 5a): T2W axial (panel a) and sagittal (panel b) images showing heterogeneously hyperintense lesion suggestive of ganglioglioma of right temporal lobe. (Panel c) shows ictal EEG buildup of rhythmic discharges from right anterior and mid temporal regions EEG = Electroencephalography

(b) (Case 5b): Ganglioglioma: tumor shows aggregates of ganglion cells (a, arrow) in a fibrillary stroma. GFAP highlights glial component (b), and synaptophysin labels the dysplastic ganglion cells (c, arrow). (A: H and E × Obj.20; B: GFAP immunoperoxidase × Obj.10; C: Synaptophysin immunoperoxidase × Obj.40) GFAP = Glial fibrillary acidic protein, H and E = Hematoxylin and eosin

(Case 6): T2W axial (panel a) and post contrast T1W (panel b) images showing small septated well-defined hyperintense lesion with absence of contrast enhancement suggestive of left inferior temporal gyrus DNET. (Panel c) shows slowing in the left temporal region (T1, T3, and T5) in the ictal EEG, DNET = Dysembryoplastic neuroepithelial tumors, EEG = Electroencephalography

(Case 7a): Axial gradient image (panel a) reveals well-defined lesion in the right hippocampus with prominent blooming and T1 FSE axial image (panel b) a peripheral rim of “popcorn” appearance suggestive of cavernoma, FSE = Fast spin echo

(Case 7b): Hippocampal cavernoma: Large fibrosed lesion within hippocampus (a: arrow). Close-up view shows cavernoma with several dilated thin venous channels (b). (A: H and E × 8, B: Masson trichrome × Obj.20), H and E = Hematoxylin and eosin

(Case 8): MRI of the brain (panel a) shows atrophy involving the right hemisphere with focal areas of hyperintensity; EEG (panel b) shows slowing of background activity (R) on right hemisphere with epileptiform discharges. Panel C shows hemispherectomy specimen showing microglial nodules in gray matter of temporal cortex (A), infiltration by cytotoxic T cells (B), and reactive astrocytosis (c) suggestive of Rasmussen encephalitis (A: H and E × Obj.20; B: CD8 immunoperoxidase × Obj.10; C: GFAP immunoperoxidase × Obj.40), MRI = Magnetic resonance imaging, EEG = Electroencephalography, H and E = Hematoxylin and eosin, GFAP = Glial fibrillary acidic protein
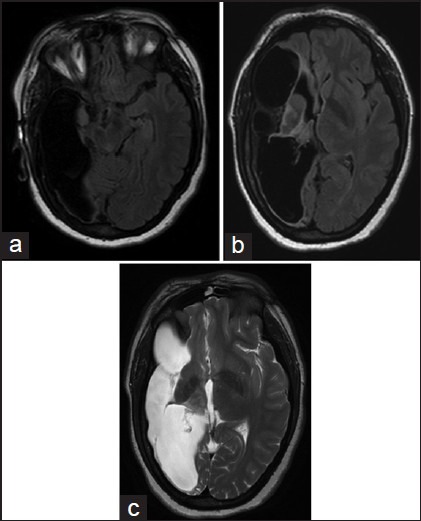
(Case 9): T1 axial (panel a), FLAIR (panel b), and T2 axial (panel c) images of a case of MCA territory infarct with gliosis, FLAIR = Fluid attenuated inversion recovery
Similar articles
-
Advances in the Surgical Management of Epilepsy: Drug-Resistant Focal Epilepsy in the Adult Patient.Neurol Clin. 2021 Feb;39(1):181-196. doi: 10.1016/j.ncl.2020.09.010. Epub 2020 Nov 7. Neurol Clin. 2021. PMID: 33223082 Review.
-
Health Technology Assessment report on the presurgical evaluation and surgical treatment of drug-resistant epilepsy.Epilepsia. 2013 Oct;54 Suppl 7:49-58. doi: 10.1111/epi.12309. Epilepsia. 2013. PMID: 24099055 Review.
-
Magnetic source imaging in presurgical evaluation of paediatric focal drug-resistant epilepsy and its predictive value of surgical outcome in lesional cases: A single-centre experience from South India.Seizure. 2021 Oct;91:22-28. doi: 10.1016/j.seizure.2021.05.015. Epub 2021 May 24. Seizure. 2021. PMID: 34058605
-
[Changes of the outcomes of epilepsy surgery within 10 years in the National Institute of Clinical Neurosciences, Hungary].Orv Hetil. 2021 Feb 7;162(6):219-226. doi: 10.1556/650.2021.31991. Orv Hetil. 2021. PMID: 33550274 Hungarian.
-
Evaluation of magnetic resonance imaging-negative drug-resistant epilepsy.Ann Indian Acad Neurol. 2014 Mar;17(Suppl 1):S80-8. doi: 10.4103/0972-2327.128667. Ann Indian Acad Neurol. 2014. PMID: 24791094 Free PMC article.
Cited by
-
Utility of 7 Tesla Magnetic Resonance Imaging in Patients With Epilepsy: A Systematic Review and Meta-Analysis.Front Neurol. 2021 Mar 19;12:621936. doi: 10.3389/fneur.2021.621936. eCollection 2021. Front Neurol. 2021. PMID: 33815251 Free PMC article.
References
-
- Engel J., Jr Surgery for seizures. N Engl J Med. 1996;334:647–52. - PubMed
-
- Spencer S, Huh L. Outcomes of epilepsy surgery in adults and children. Lancet Neurol. 2008;7:525–37. - PubMed
-
- McKhann GM, 2nd, Bourgeois BF, Goodman RR. Epilepsy surgery: Indications, approaches, and results. Semin Neurol. 2002;22:269–78. - PubMed
-
- Schuele SU, Lüders HO. Intractable epilepsy: Management and therapeutic alternatives. Lancet Neurol. 2008;7:514–24. - PubMed
-
- Engel J, Wiebe S, French J, Sperling M, Williamson P, Spencer D, et al. Quality Standards Subcommittee of the American Academy of Neurology, American Epilepsy Society, American Association of Neurological Surgeons. Practice parameter: Temporal lobe and localized neocortical resections for epilepsy: Report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60:538–47. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
