

Positive end-expiratory pressure attenuates positional effect after thoracotomy
- PMID: 24791175
- PMCID: PMC4005157
- DOI: 10.4103/1817-1737.128860
Positive end-expiratory pressure attenuates positional effect after thoracotomy
Abstract
Context: Thoracotomy is a common procedure. However, thoracotomy leads to lung atelectasis and deteriorates pulmonary gas exchange in operated side. Therefore, different positions with operated side lowermost or uppermost may lead to different gas exchange after thoracotomy. Besides, PEEP (positive end-expiratory pressure) influence lung atelectasis and should influence gas exchange.
Aims: The purpose of this study was to determine the physiological changes in different positions after thoracotomy. In addition, we also studied the influence of PEEP to positional effects after thoracotomy.
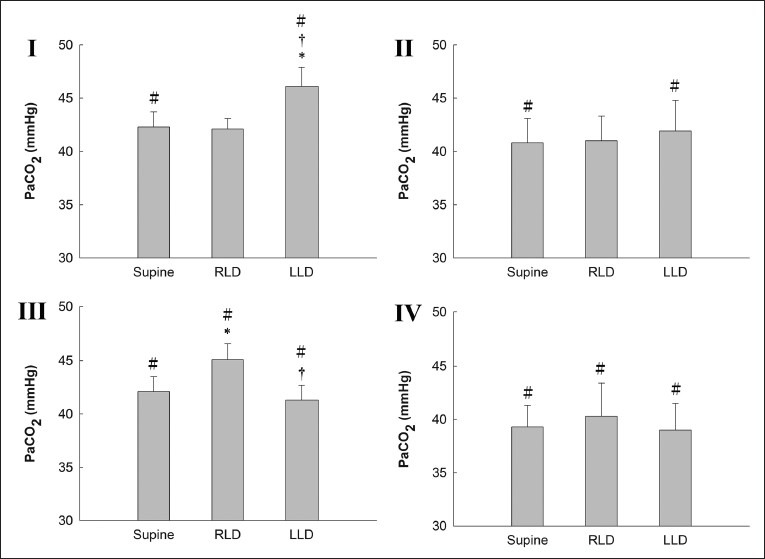
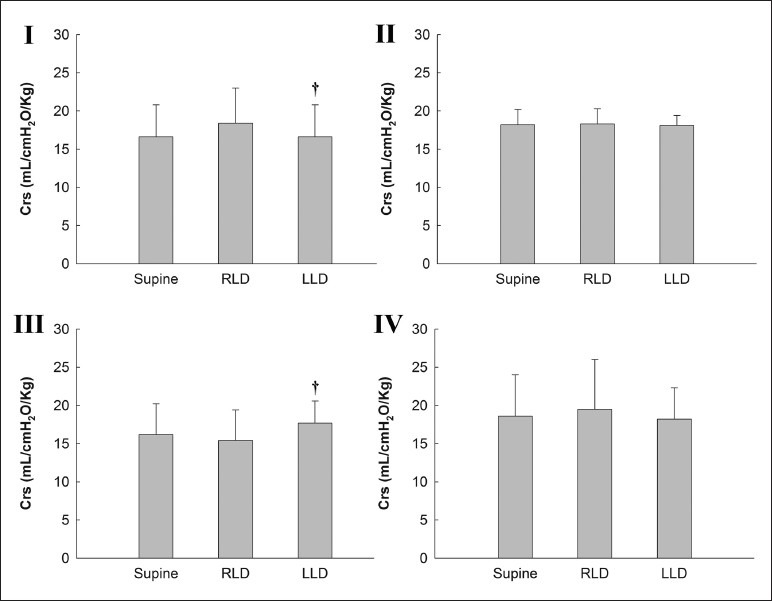
Materials and methods: There were eight pigs in each group. Group I received left thoracotomy with zero end-expiratory pressure (ZEEP), and group II with PEEP; group III received right thoracotomy with ZEEP and group IV with PEEP. We changed positions to supine, LLD (left lateral decubitus) and RLD (right lateral decubitus) in random order after thoracotomy.
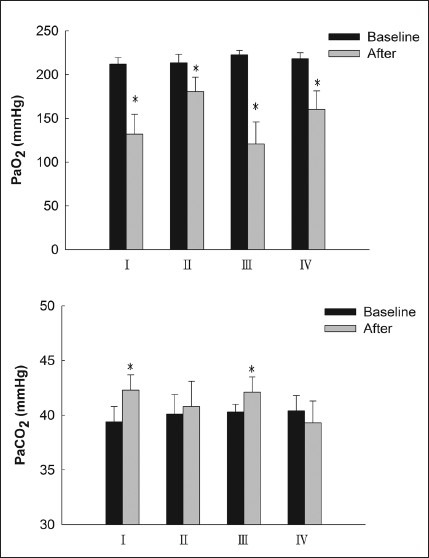
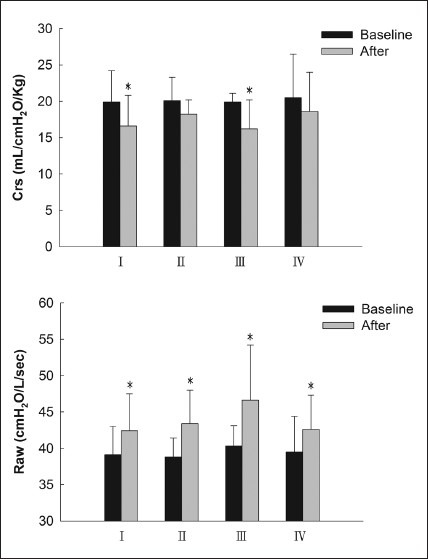
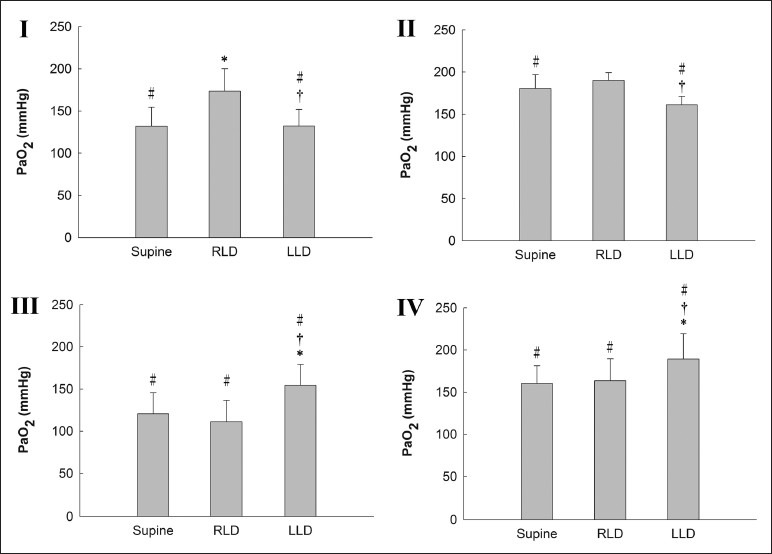
Results: PaO2 was decreased after thoracotomy and higher in RLD after left thoracotomy and in LLD after right thoracotomy. PaO2 in groups II and IV was higher than in groups I and III if with the same position. In group I and III, PaCO2 was increased after thoracotomy and was higher in LLD after left thoracotomy and in RLD after right thoracotomy. In groups II and IV, there were no PaCO2 changes in different positions after thoracotomy. Lung compliance (Crs) was decreased after thoracotomy in groups I and III and highest in RLD after left thoracotomy and in LLD after right thoracotomy. In groups II and IV, there were no changes in Crs regardless of the different positions.
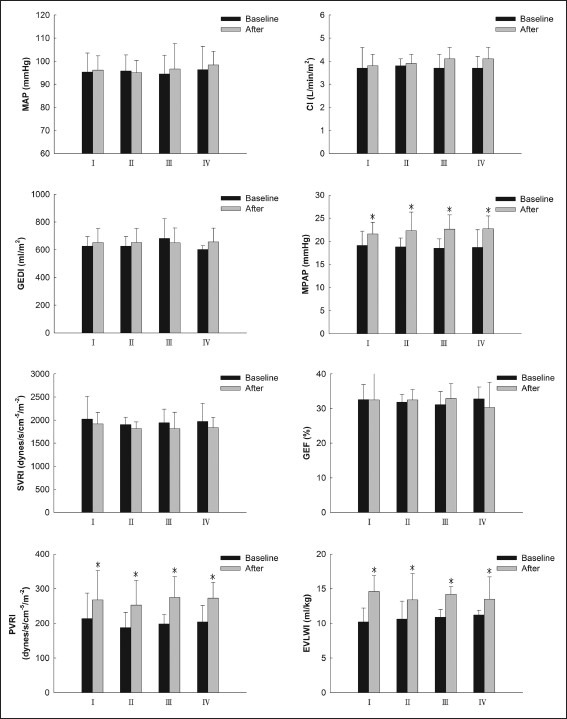
Conclusion: There were significant changes with regards to pulmonary gas exchange, hemodynamics and Crs after thoracotomy. The best position was non-operated lung lowermost Applying PEEP attenuates the positional effects.
Keywords: Positive end-expiratory pressure; position; pulmonary gas exchange; thoracotomy.
Conflict of interest statement
Figures
Similar articles
-
Effect of body positions on hemodynamics and gas exchange in anesthetized pigs shortly after pneumonectomy.Shock. 2010 Nov;34(5):482-7. doi: 10.1097/SHK.0b013e3181dc0812. Shock. 2010. PMID: 20220567
-
Positional hypoxaemia following post-traumatic pulmonary insufficiency.Can Anaesth Soc J. 1977 May;24(3):346-52. doi: 10.1007/BF03005107. Can Anaesth Soc J. 1977. PMID: 326354
-
Positive end-expiratory pressure applied to the dependent lung during one-lung ventilation improves oxygenation and respiratory mechanics in patients with high FEV1.Eur J Anaesthesiol. 2004 Dec;21(12):938-43. doi: 10.1017/s0265021504000316. Eur J Anaesthesiol. 2004. PMID: 15719856 Clinical Trial.
-
Effects of positive end-expiratory pressure on anesthesia-induced atelectasis and gas exchange in anesthetized and mechanically ventilated sheep.Am J Vet Res. 2010 Aug;71(8):867-74. doi: 10.2460/ajvr.71.8.867. Am J Vet Res. 2010. PMID: 20673084
-
Prospective, randomized, controlled evaluation of the preventive effects of positive end-expiratory pressure on patient oxygenation during one-lung ventilation.Eur J Anaesthesiol. 2003 Sep;20(9):704-10. doi: 10.1017/s0265021503001145. Eur J Anaesthesiol. 2003. PMID: 12974591 Clinical Trial.
References
-
- Dubose J, Inaba K, Demetriades D, Scalea TM, O’connor J, Menaker J, et al. Management of post-traumatic retained hemothorax: A prospective, observational, multicenter AAST study. J Trauma. 2012;72:11–24. - PubMed
-
- Howington JA, Gunnarsson CL, Maddaus MA, McKenna RJ, Meyers BF, Miller D, et al. In-hospital clinical and economic consequences of pulmonary wedge resections for cancer using video-assisted thoracoscopic techniques vs traditional open resections: A retrospective database analysis. Chest. 2012;141:429–35. - PubMed
-
- Onat S, Ulku R, Avci A, Ates G, Ozcelik C. Urgent thoracotomy for penetrating chest trauma: Analysis of 158 patients of a single center. Injury. 2011;42:900–4. - PubMed
-
- Rustomjee T, Wagner A, Orton EC. Effect of 5 cm of water positive end-expiratory pressure on arterial oxygen tension in dogs during and after thoracotomy. Vet Surg. 1994;23:307–10. - PubMed
-
- Licker M, Fauconnet P, Villiger Y, Tschopp JM. Acute lung injury and outcomes after thoracic surgery. Curr Opin Anaesthesiol. 2009;22:61–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
