

Prognostic significance of clinical, histopathological, and molecular characteristics of medulloblastomas in the prospective HIT2000 multicenter clinical trial cohort
- PMID: 24791927
- PMCID: PMC4059991
- DOI: 10.1007/s00401-014-1276-0
Prognostic significance of clinical, histopathological, and molecular characteristics of medulloblastomas in the prospective HIT2000 multicenter clinical trial cohort
Abstract
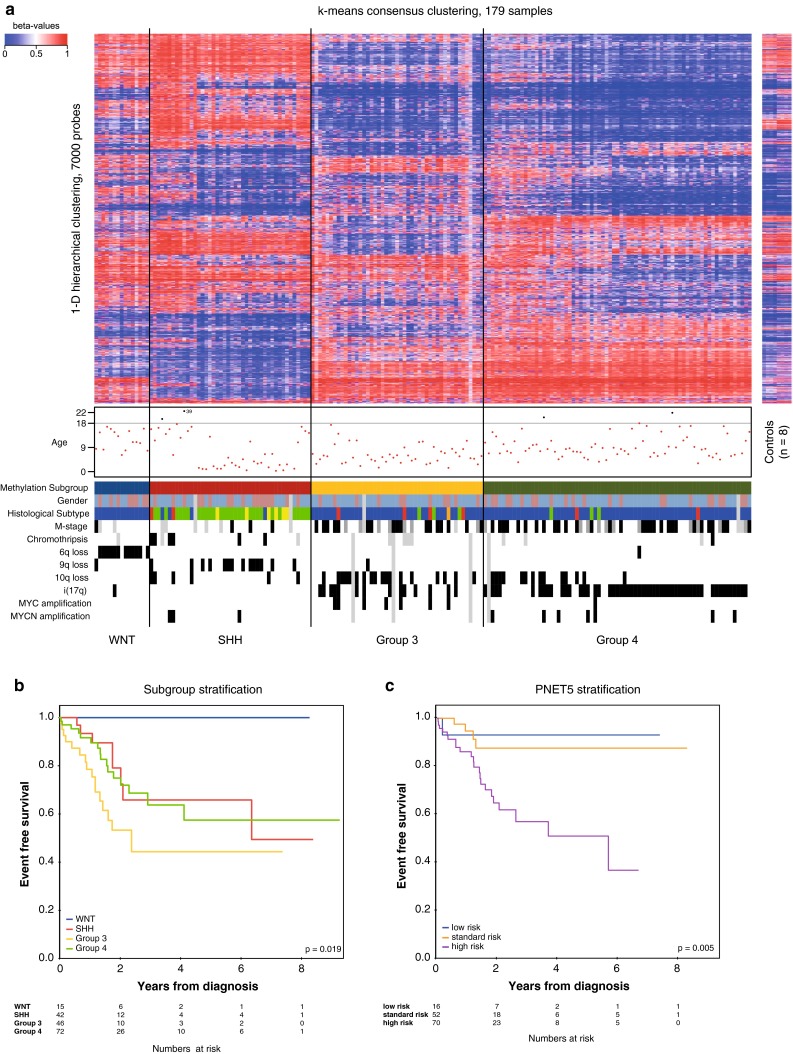
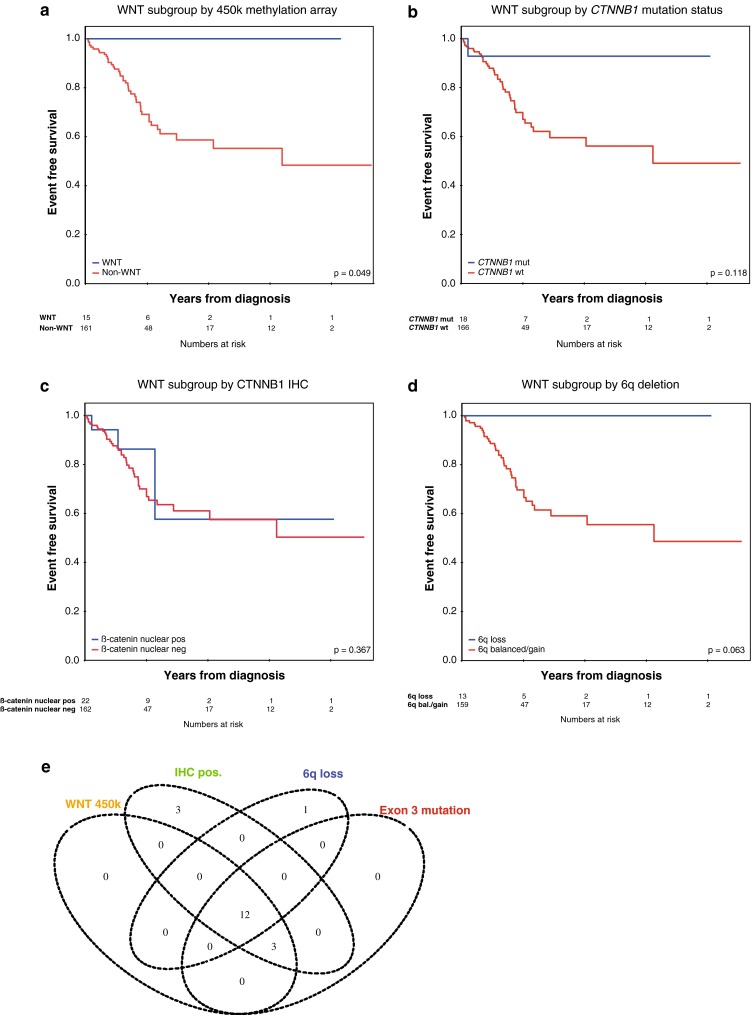
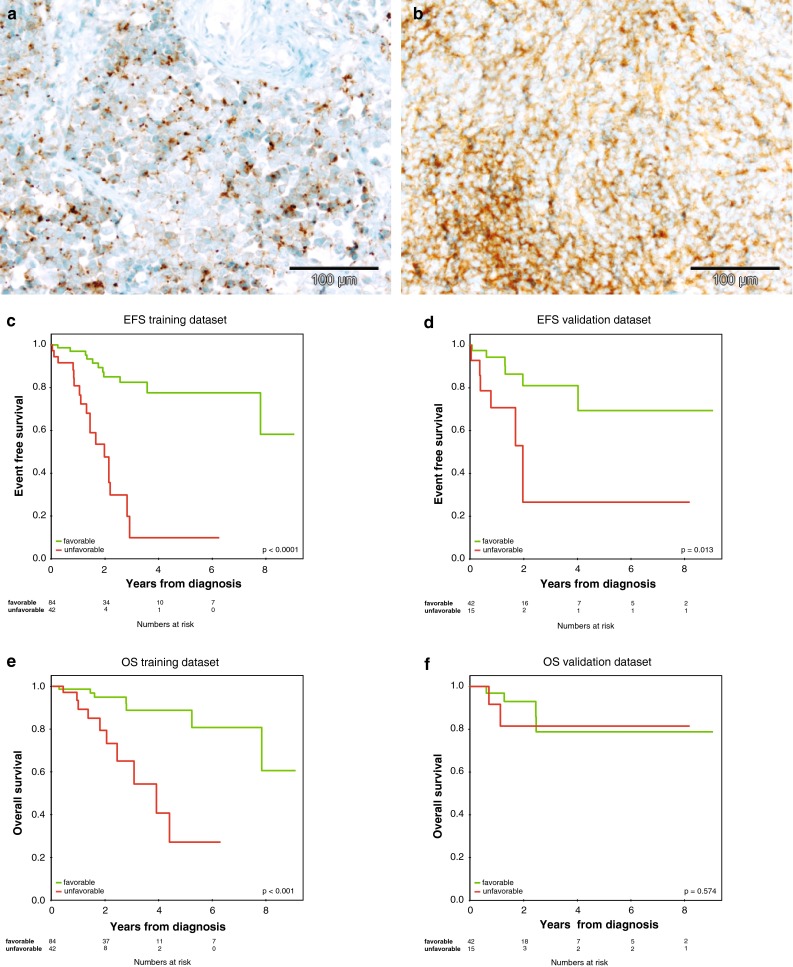
This study aimed to prospectively evaluate clinical, histopathological and molecular variables for outcome prediction in medulloblastoma patients. Patients from the HIT2000 cooperative clinical trial were prospectively enrolled based on the availability of sufficient tumor material and complete clinical information. This revealed a cohort of 184 patients (median age 7.6 years), which was randomly split at a 2:1 ratio into a training (n = 127), and a test (n = 57) dataset in order to build and test a risk score for this population. Independent validation was performed in a non-overlapping cohort (n = 83). All samples were subjected to thorough histopathological investigation, CTNNB1 mutation analysis, quantitative PCR, MLPA and FISH analyses for cytogenetic variables, and methylome analysis. By univariable analysis, clinical factors (M-stage), histopathological variables (large cell component, endothelial proliferation, synaptophysin pattern), and molecular features (chromosome 6q status, MYC amplification, subgrouping) were found to be prognostic. Molecular consensus subgrouping (WNT, SHH, Group 3, Group 4) was validated as an independent feature to stratify patients into different risk groups. When comparing methods for the identification of WNT-driven medulloblastoma, this study identified CTNNB1 sequencing and methylation profiling to most reliably identify these patients. After removing patients with particularly favorable (CTNNB1 mutation, extensive nodularity) or unfavorable (MYC amplification) markers, a risk score for the remaining "intermediate molecular risk" population dependent on age, M-stage, pattern of synaptophysin expression, and MYCN copy-number status was identified, with speckled synaptophysin expression indicating worse outcome. Test and independent validation of the score confirmed significant discrimination of patients by risk profile. Methylation subgrouping and CTNNB1 mutation status represent robust tools for the risk stratification of medulloblastoma. A simple clinico-pathological risk score was identified, which was confirmed in a test set and by independent clinical validation.
Figures
References
-
- Dahmen RP, Koch A, Denkhaus D, et al. Deletions of AXIN1, a component of the WNT/wingless pathway, in sporadic medulloblastomas. Cancer Res. 2001;61(19):7039–7043. - PubMed
-
- Gajjar A, Chintagumpala M, Ashley D, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol. 2006;7(10):813–820. doi: 10.1016/S1470-2045(06)70867-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
