

Clinical manifestations of lead-dependent infective endocarditis: analysis of 414 cases
- PMID: 24791953
- PMCID: PMC4129226
- DOI: 10.1007/s10096-014-2117-8
Clinical manifestations of lead-dependent infective endocarditis: analysis of 414 cases
Abstract
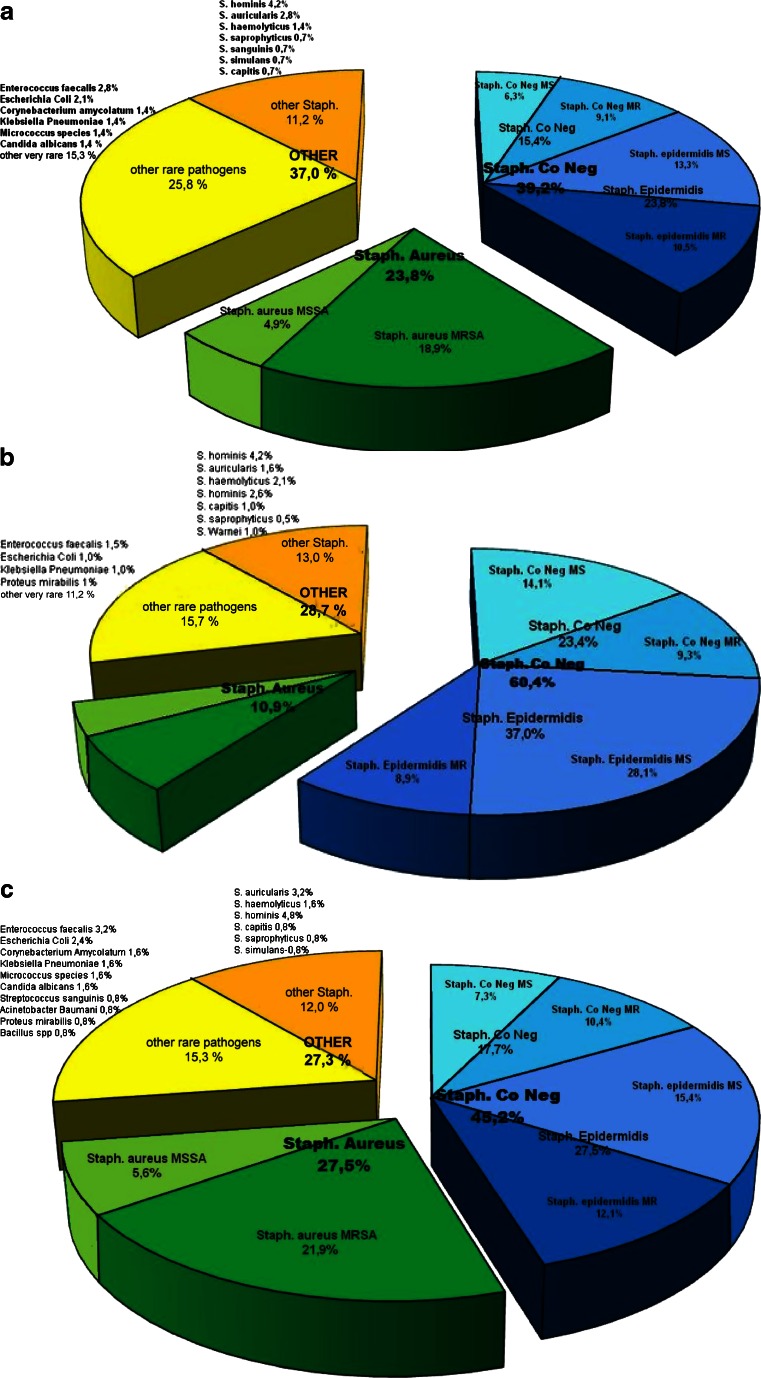
It is important to identify clinical manifestations of lead-dependent infective endocarditis (LDIE), as it begins insidiously with the slow development of nonspecific symptoms. Clinical data from 414 patients with the diagnosis of LDIE according to Modified Duke Lead Criteria (MDLC) were analyzed. Patients with LDIE had been identified in a population of 1,426 subjects submitted to transvenous lead extraction (TLE) in the Reference Clinical Cardiology Center in Lublin between 2006 and 2013. The symptoms of LDIE and pocket infection were detected in 62.1 % of patients. The mean duration of LDIE symptoms prior to referral for TLE was 6.7 months. Fever and shivers were found in 55.3 % of patients, and pulmonary infections in 24.9 %. Vegetations were detected in 67.6 % of patients, and positive cultures of blood, lead, and pocket in 34.5, 46.4, and 30.0 %, respectively. The most common pathogens in all type cultures were coagulase-negative staphylococci (CNS), with Staphylococcus epidermidis domination; the second most common organism was Staphylococcus aureus. 76.3 % of patients were treated with empirical antibiotic therapy before hospitalization due to TLE. In the laboratory tests, the mean white blood cell count was 9,671 ± 5,212/μl, mean erythrocyte sedimentation rate 43 mm, C-reactive protein (CRP) 46.3 mg/dl ± 61, and procalcitonin 1.57 ± 4.4 ng/ml. The multivariate analysis showed that the probability of LDIE increased with increasing CRP. The diagnosis of LDIE based on MDLC may be challenging because of a relatively low sensitivity of major criteria, which is associated with early antibiotic therapy and low usefulness of minor criteria. The important clinical symptoms of LDIE include fever with shivering and recurrent pulmonary infections. The most specific pathogens were Staphylococcus epidermidis and Staphylococcus aureus. Laboratory tests most frequently revealed normal white blood cell count, relatively rarely elevated procalcitonin level, and significantly increased erythrocyte sedimentation rate (ESR) and CRP. This constellation of signs should prompt a more thorough search for LDIE.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
