

Giant left paraduodenal hernia
- PMID: 24792018
- PMCID: PMC4025259
- DOI: 10.1136/bcr-2013-202465
Giant left paraduodenal hernia
Abstract
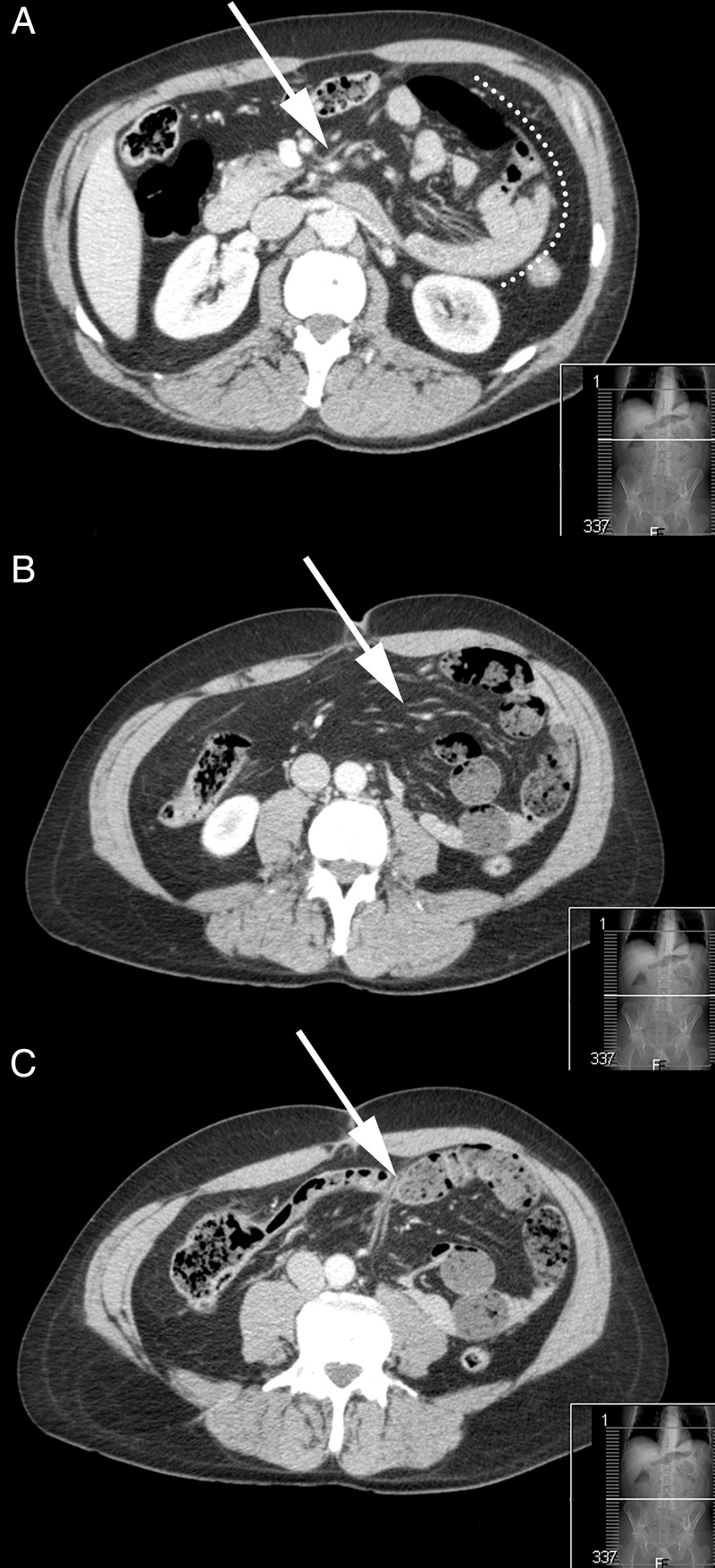
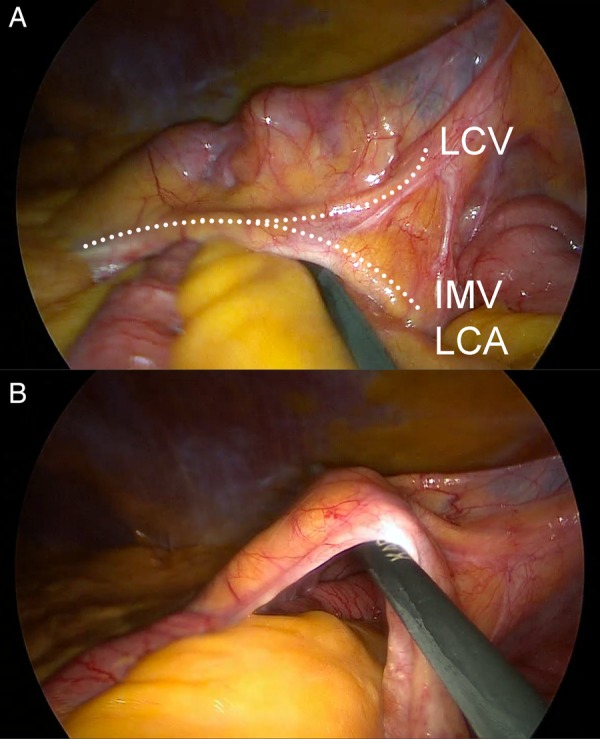
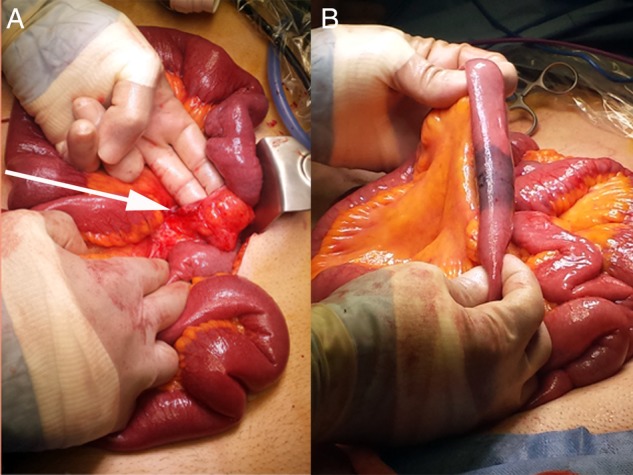
Left paraduodenal hernia (LPDH) is a retrocolic internal hernia of congenital origin that develops through the fossa of Landzert, and extends into the descending mesocolon and left portion of the transverse mesocolon. It carries significant overall risk of mortality, yet delay in diagnosis is not unusual due to subtle and elusive features. Familiarisation with the embryological and anatomical features of this rare hernia is essential for surgical management. This is especially important with respect to vascular anatomy as major mesenteric vessels form intimate relationships with the ventral rim and anterior portion of the hernia. As an illustrative case, we describe our experience with a striking example of LPDH, particularly focusing on the inherent diagnostic challenges and associated critical vascular anatomy. We advocate the role of diagnostic laparoscopy; however caution that decision to safely proceed with laparoscopic repair must occur only with confident identification of the vascular anatomy involved.
Figures

Similar articles
-
Left Paraduodenal Hernia.J Gastrointest Surg. 2018 May;22(5):925-927. doi: 10.1007/s11605-017-3626-4. Epub 2017 Nov 20. J Gastrointest Surg. 2018. PMID: 29159758
-
[Left-sided paraduodenal hernia].Rozhl Chir. 1980 Jun;59(6):415-8. Rozhl Chir. 1980. PMID: 7403966 Czech. No abstract available.
-
Diagnostic laparoscopy and laparoscopic repair of a left paraduodenal hernia can shorten hospital stay.JSLS. 2006 Jan-Mar;10(1):90-3. JSLS. 2006. PMID: 16709368 Free PMC article.
-
[Left paraduodenal hernia: a case report and review of the literature].Chir Ital. 2008 Sep-Oct;60(5):721-4. Chir Ital. 2008. PMID: 19062496 Review. Italian.
-
Left paraduodenal hernia: case report and review of the literature.BMJ Case Rep. 2010 Nov 23;2010:bcr0420102936. doi: 10.1136/bcr.04.2010.2936. BMJ Case Rep. 2010. PMID: 22797200 Free PMC article. Review.
Cited by
-
Paraduodenal hernias: a systematic review of the literature.Hernia. 2019 Dec;23(6):1187-1197. doi: 10.1007/s10029-019-01947-3. Epub 2019 Apr 20. Hernia. 2019. PMID: 31006063
-
A late presentation of a left paraduodenal hernia in an elderly patient admitted in emergency: A case report.Radiol Case Rep. 2024 Jan 15;19(4):1356-1360. doi: 10.1016/j.radcr.2024.01.013. eCollection 2024 Apr. Radiol Case Rep. 2024. PMID: 38288049 Free PMC article.
-
Laparoscopic correction of hydronephrosis caused by left paraduodenal hernia in a child with cryptorchism: A case report.World J Clin Cases. 2022 Sep 26;10(27):9814-9820. doi: 10.12998/wjcc.v10.i27.9814. World J Clin Cases. 2022. PMID: 36186215 Free PMC article.
-
Paraduodenal hernias in children: Etiology, treatment, and outcomes of a rare but real cause of bowel obstruction.Int J Surg Case Rep. 2019;64:105-108. doi: 10.1016/j.ijscr.2019.10.001. Epub 2019 Oct 10. Int J Surg Case Rep. 2019. PMID: 31627058 Free PMC article.
-
Large left paraduodenal hernia with intestinal ischemia: a case report and literature review.J Int Med Res. 2020 Sep;48(9):300060520955040. doi: 10.1177/0300060520955040. J Int Med Res. 2020. PMID: 32938278 Free PMC article. Review.
References
-
- Meyers MA. Paraduodenal hernias. Radiologic and arteriographic diagnosis. Radiology 1970;95:29–37 - PubMed
-
- Falk GA, Yurcisin BJ, Sell HS. Left paraduodenal hernia: case report and review of the literature. BMJ Case Rep 2010;2010,pii:bcr0420102936. 10.1136/bcr.04.2010.2936 - DOI - PMC - PubMed
-
- Brigham RA, Fallon WF, Saunders JR, et al. Paraduodenal hernia: diagnosis and surgical management. Surgery 1984;96:498–502 - PubMed
-
- Blachar A, Federle MP, Dodson SF. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology 2001;218:68–74 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials