

Radiologic manifestations of angioedema
- PMID: 24792779
- PMCID: PMC4035492
- DOI: 10.1007/s13244-014-0329-1
Radiologic manifestations of angioedema
Abstract
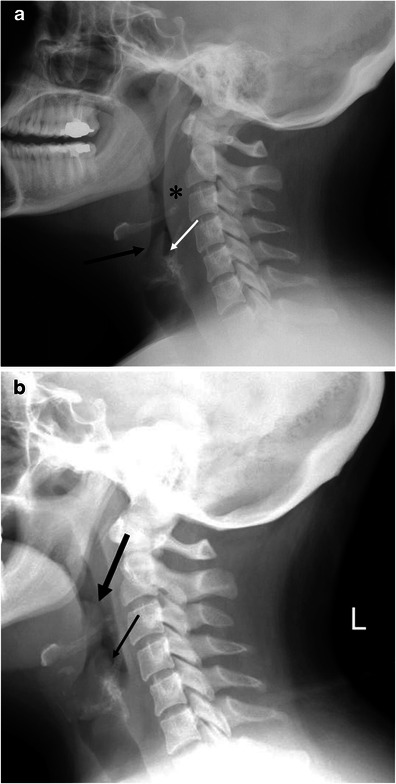
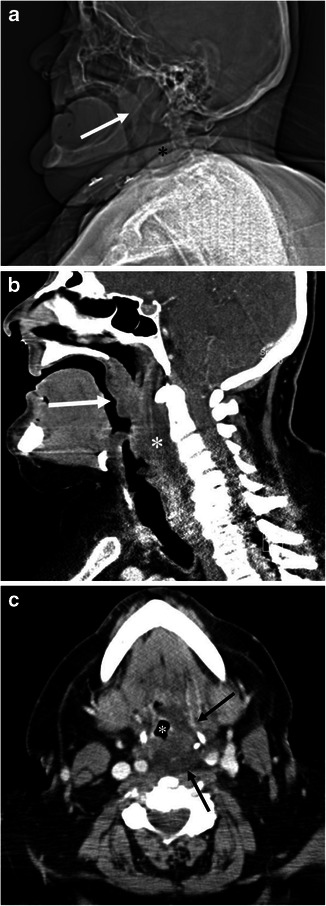
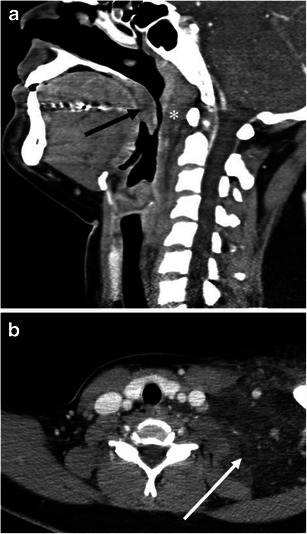
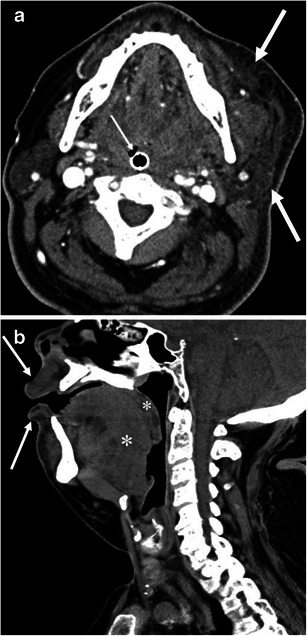
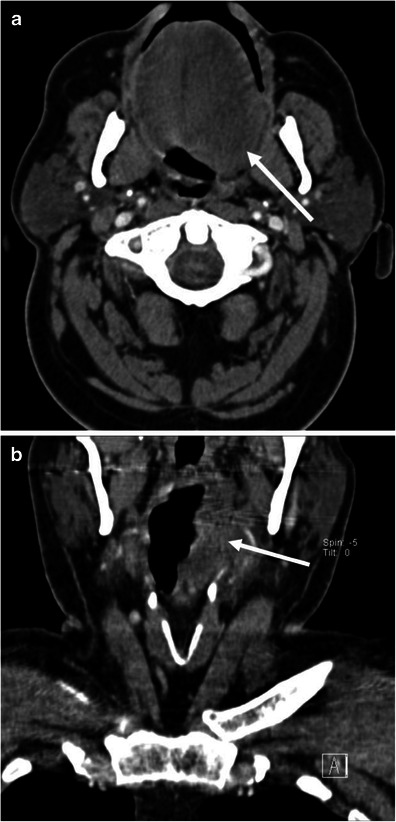
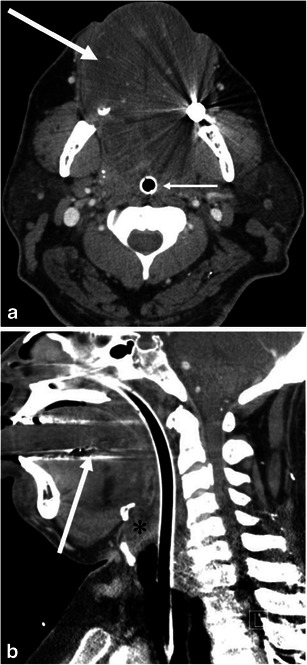
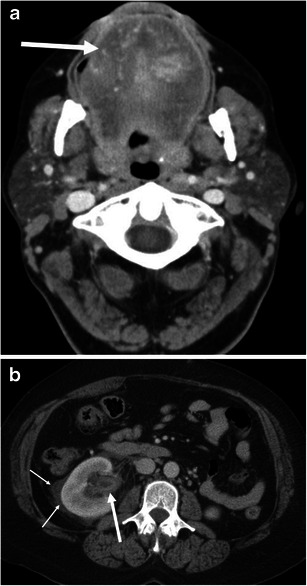
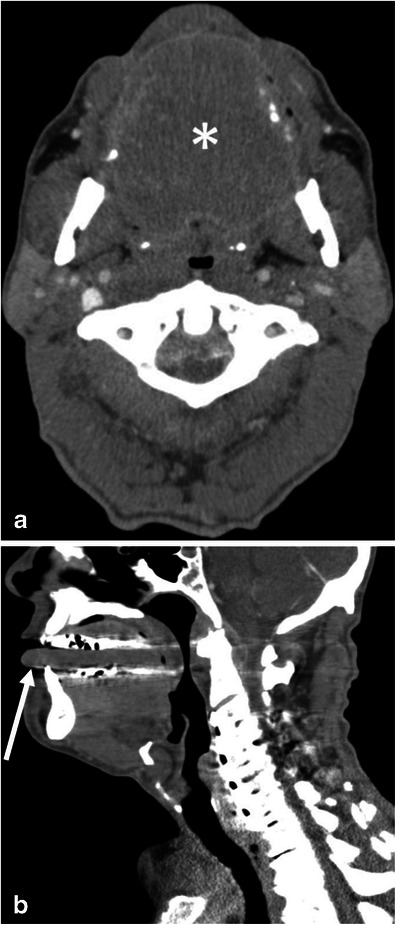
Objectives: The purpose of this pictorial review is to present imaging findings of angioedema involving the various organs.
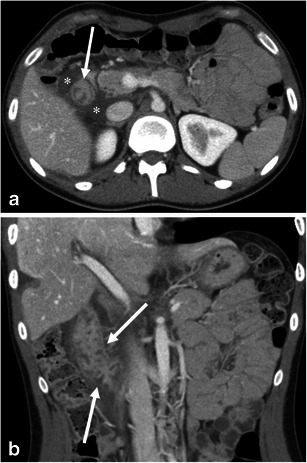
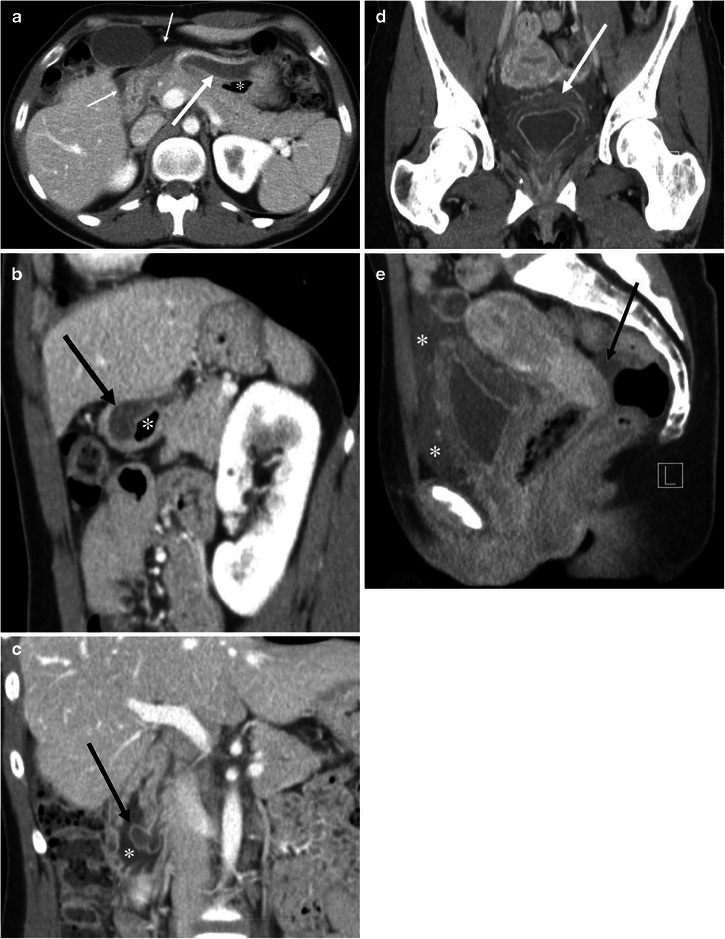
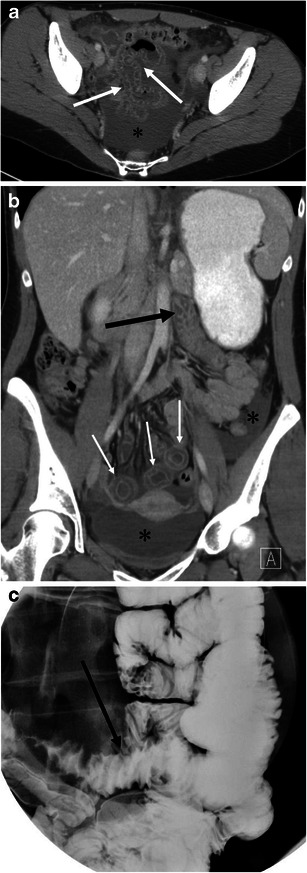
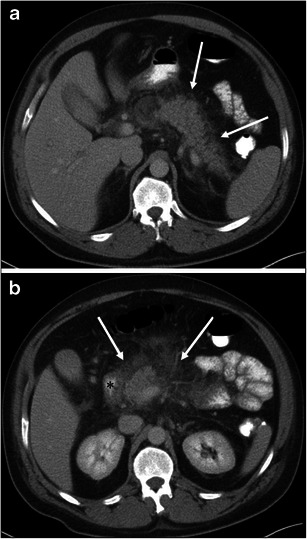
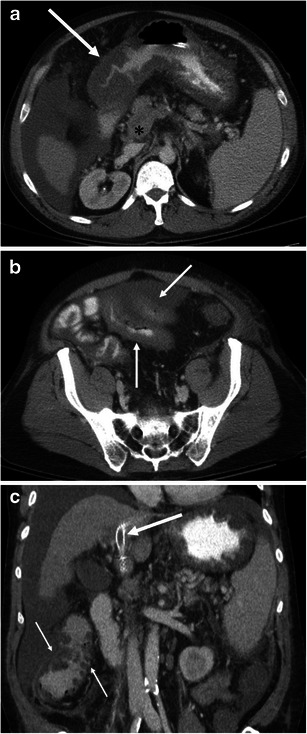
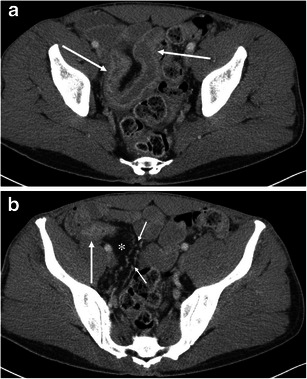
Conclusion: The role of imaging for patients with angioedema includes the evaluation of the upper airway for obstruction and the exclusion of other possible aetiologies, such as neoplastic or infectious processes. Glossomegaly is a common finding of head and neck angioedema. Angioedema may involve organ systems beyond the superficial regions and the head and neck including the gastrointestinal and genitourinary tracts. Angioedema of the visceral organs is often accompanied by adjacent fluid, and it is commonly diffuse or concentric but can also be multifocal and asymmetric.
Teaching points: • The evaluation of the upper airway obstruction is important for head and neck angioedema. • Glossomegaly with decreased attenuation is common in head and neck angioedema. • Angioedema of the visceral organs can be multifocal and asymmetric. • Angioedema of the visceral organs is often accompanied by adjacent fluid. • It is important to include clinical and laboratory findings for the diagnosis of angioedema.
Figures
References
-
- Quinke HE. Über akutes umschriebenes Hautödem. Monatsh Prakt Dermatol. 1882;1:129–131.
LinkOut - more resources
Full Text Sources
Other Literature Sources
