

Association of hypometabolism and amyloid levels in aging, normal subjects
- PMID: 24793183
- PMCID: PMC4105262
- DOI: 10.1212/WNL.0000000000000467
Association of hypometabolism and amyloid levels in aging, normal subjects
Abstract
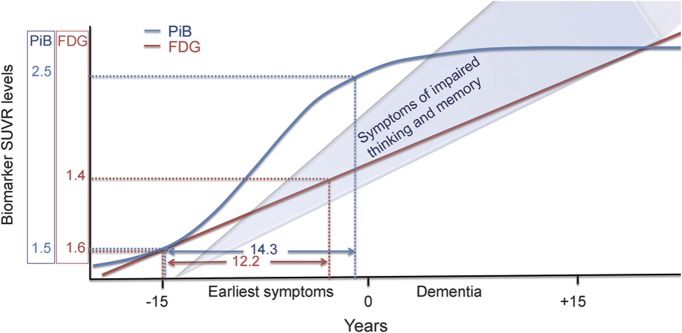
Objective: We evaluated the relationship of amyloid, seen on Pittsburgh compound B (PiB)-PET, and metabolism, seen on [(18)F]-fluorodeoxyglucose (FDG)-PET, in normal subjects to better understand pathogenesis and biomarker selection in presymptomatic subjects.
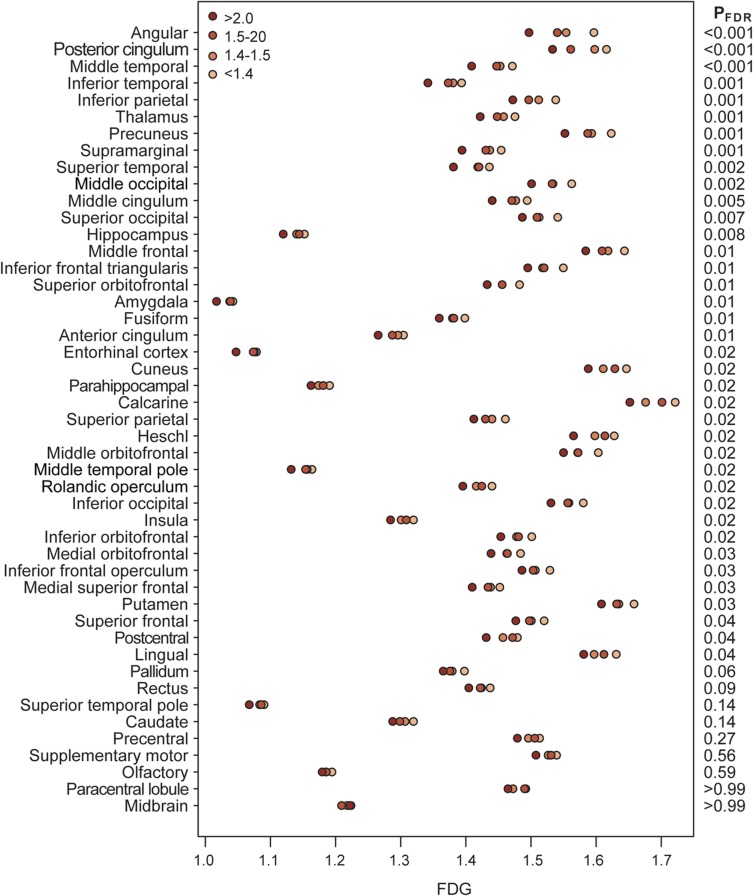
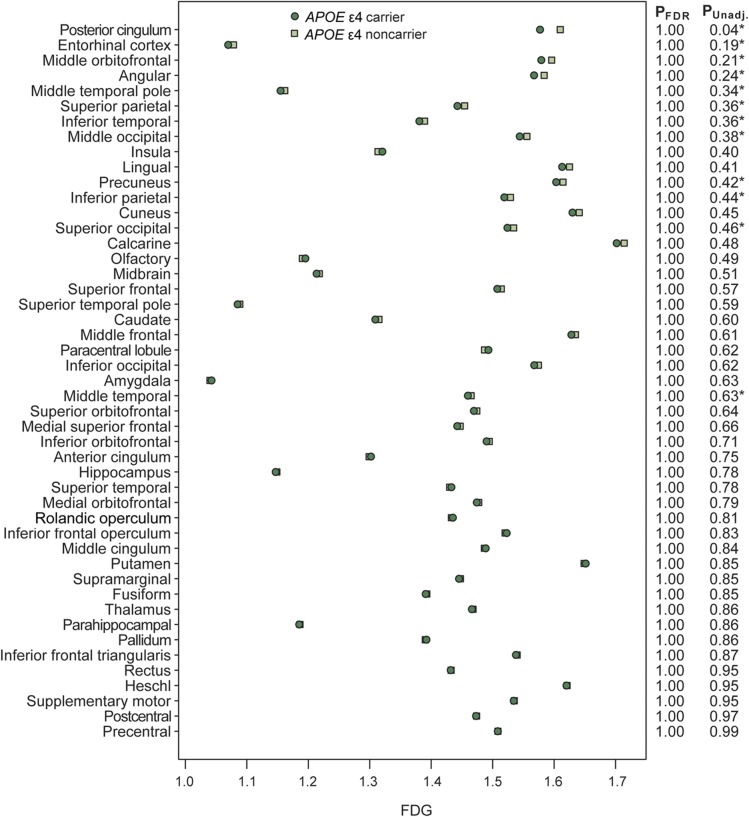
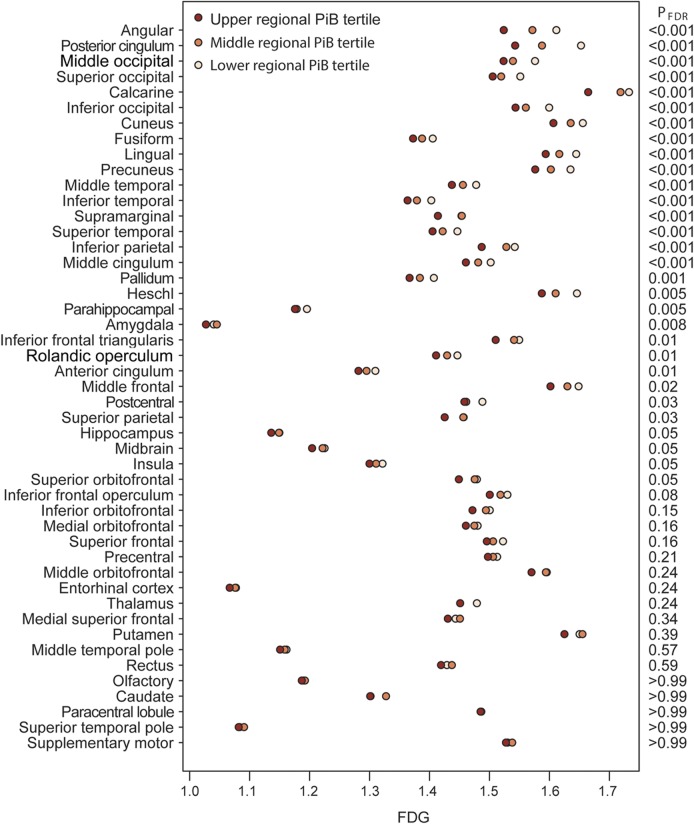
Methods: Normal participants (aged 70-95 years; 600 with PiB-PET, FDG-PET, and MRI) were included. We performed a cross-sectional evaluation and subcategorized participants into amyloid-negative (<1.4), high-normal (1.4-1.5), positive (1.5-2.0), and markedly positive (>2.0) PiB standardized uptake value ratio groups representing different levels of amyloid brain load. Associations with metabolism were assessed in each group. Relationships with APOE ε4 carriage were evaluated.
Results: Hypometabolism in "Alzheimer disease (AD)-signature" regions was strongly associated with PiB load. Hypometabolism was greater with more positive PiB levels. Additional, more-diffuse cortical hypometabolism was also found to be associated with PiB, although less so. No hypermetabolism was seen in any subset. No significant incremental hypometabolism was seen in APOE-positive vs -negative subjects.
Conclusions: Hypometabolism in PiB-positive, cognitively normal subjects in a population-based cohort occurs in AD-signature cortical regions and to a lesser extent in other cortical regions. It is more pronounced with higher amyloid load and supports a dose-dependent association. The effect of APOE ε4 carriage in this group of subjects does not appear to modify their hypometabolic "AD-like" neurodegeneration. Consideration of hypometabolism associated with amyloid load may aid trials of AD drug therapy.
© 2014 American Academy of Neurology.
Figures
References
-
- Villemagne VL, Burnham S, Bourgeat P, et al. Amyloid beta deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer's disease: a prospective cohort study. Lancet Neurol 2013;12:357–367 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous