

Outcomes in African Americans undergoing cardioverter-defibrillator implantation for primary prevention of sudden cardiac death: findings from the Prospective Observational Study of Implantable Cardioverter-Defibrillators (PROSE-ICD)
- PMID: 24793459
- PMCID: PMC4108523
- DOI: 10.1016/j.hrthm.2014.04.039
Outcomes in African Americans undergoing cardioverter-defibrillator implantation for primary prevention of sudden cardiac death: findings from the Prospective Observational Study of Implantable Cardioverter-Defibrillators (PROSE-ICD)
Abstract
Background: Implantable cardioverter-defibrillators (ICDs) reduce the risk of death in patients with left ventricular dysfunction. Little is known regarding the benefit of this therapy in African Americans (AAs).
Objective: The purpose of this study was to determine the association between AA race and outcomes in a cohort of primary prevention ICD patients.
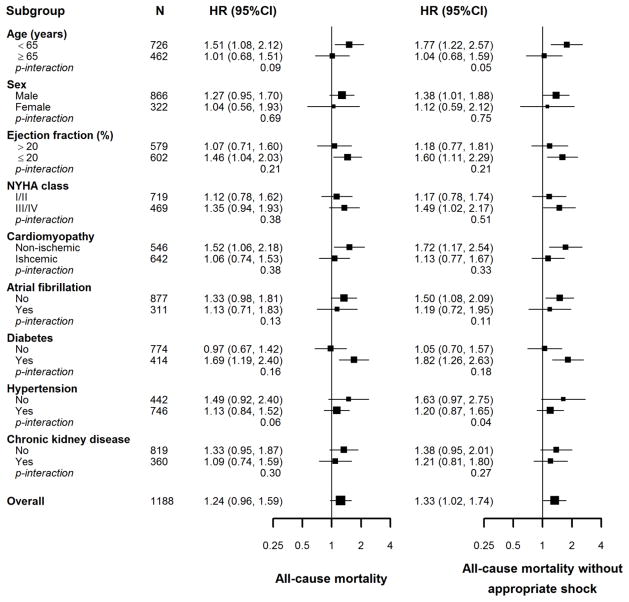
Methods: We conducted a prospective cohort study of patients with systolic heart failure who underwent ICD implantation for primary prevention of sudden cardiac death. The primary end-point was appropriate ICD shock defined as a shock for rapid ventricular tachyarrhythmias. The secondary end-point was all-cause mortality.
Results: There were 1189 patients (447 AAs and 712 non-AAs) enrolled. Over a median follow-up of 5.1 years, a total of 137 patients experienced an appropriate ICD shock, and 343 died (294 of whom died without receiving an appropriate ICD shock). The multivariate adjusted hazard ratio (95% confidence interval) comparing AAs vs non-AAs were 1.24 (0.96-1.59) for all-cause mortality, 1.33 (1.02, 1.74) for all-cause mortality without receiving appropriate ICD shock, and 0.78 (0.51, 1.19) for appropriate ICD shock. Ejection fraction, diabetes, and hypertension appeared to explain 24.1% (10.1%-69.5%), 18.7% (5.3%-58.0%), and 13.6% (3.8%-53.6%) of the excess risk of mortality in AAs, with a large proportion of the mortality difference remaining unexplained.
Conclusion: In patients with primary prevention ICDs, AAs had an increased risk of dying without receiving an appropriate ICD shock compared to non-AAs.
Keywords: African American; All-cause mortality; Implantable cardioverter-defibrillator; Sudden cardiac death; implantable cardioverter-defibrillator shock.
Copyright © 2014 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Protein biomarkers identify patients unlikely to benefit from primary prevention implantable cardioverter defibrillators: findings from the Prospective Observational Study of Implantable Cardioverter Defibrillators (PROSE-ICD).Circ Arrhythm Electrophysiol. 2014 Dec;7(6):1084-91. doi: 10.1161/CIRCEP.113.001705. Epub 2014 Oct 1. Circ Arrhythm Electrophysiol. 2014. PMID: 25273351 Free PMC article.
-
Changes in Follow-Up Left Ventricular Ejection Fraction Associated With Outcomes in Primary Prevention Implantable Cardioverter-Defibrillator and Cardiac Resynchronization Therapy Device Recipients.J Am Coll Cardiol. 2015 Aug 4;66(5):524-31. doi: 10.1016/j.jacc.2015.05.057. J Am Coll Cardiol. 2015. PMID: 26227190 Free PMC article.
-
Prospective observational study of implantable cardioverter-defibrillators in primary prevention of sudden cardiac death: study design and cohort description.J Am Heart Assoc. 2013 Feb 22;2(1):e000083. doi: 10.1161/JAHA.112.000083. J Am Heart Assoc. 2013. PMID: 23525420 Free PMC article.
-
Decision-making regarding subcutaneous implantable cardioverter defibrillator as primary prevention in patients with low ejection fraction.Pacing Clin Electrophysiol. 2024 Oct;47(10):1285-1292. doi: 10.1111/pace.15065. Epub 2024 Aug 19. Pacing Clin Electrophysiol. 2024. PMID: 39161154 Review.
-
Systematic Review for the 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society.J Am Coll Cardiol. 2018 Oct 2;72(14):1653-1676. doi: 10.1016/j.jacc.2017.10.052. Epub 2017 Oct 30. J Am Coll Cardiol. 2018. PMID: 29097297
Cited by
-
Racial and ethnic differences in implantable cardioverter-defibrillator patient selection, management, and outcomes.Heart Rhythm O2. 2022 Dec 16;3(6Part B):807-816. doi: 10.1016/j.hroo.2022.09.003. eCollection 2022 Dec. Heart Rhythm O2. 2022. PMID: 36589011 Free PMC article. Review.
-
Case series of black athletes participating in sports with an implantable cardioverter-defibrillator: Data from the ICD Sports Registry.Heart Rhythm O2. 2025 Apr 24;6(7):1044-1046. doi: 10.1016/j.hroo.2025.04.008. eCollection 2025 Jul. Heart Rhythm O2. 2025. PMID: 40734739 Free PMC article. No abstract available.
-
Race, ethnicity, and the risk of sudden death<sup/>Trends Cardiovasc Med. 2019 Feb;29(2):120-126. doi: 10.1016/j.tcm.2018.07.001. Epub 2018 Jul 10. Trends Cardiovasc Med. 2019. PMID: 30029848 Free PMC article. Review.
-
Heart Failure with Improved Ejection Fraction: Insight into the Variable Nature of Left Ventricular Systolic Function.Int J Environ Res Public Health. 2022 Nov 3;19(21):14400. doi: 10.3390/ijerph192114400. Int J Environ Res Public Health. 2022. PMID: 36361280 Free PMC article. Review.
References
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002 Mar 21;346:877–883. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005 Jan 20;352:225–237. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 1999 Dec 16;341:1882–1890. - PubMed
-
- Kadish A, Dyer A, Daubert JP, et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004 May 20;350:2151–2158. - PubMed
-
- Hohnloser SH, Kuck KH, Dorian P, Roberts RS, Hampton JR, Hatala R, Fain E, Gent M, Connolly SJ. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med. 2004 Dec 9;351:2481–2488. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
