

Effect of sustaining lifestyle modifications (nonsmoking, weight reduction, physical activity, and mediterranean diet) after healing of myocardial infarction, percutaneous intervention, or coronary bypass (from the REasons for Geographic and Racial Differences in Stroke Study)
- PMID: 24793668
- PMCID: PMC4348576
- DOI: 10.1016/j.amjcard.2014.03.033
Effect of sustaining lifestyle modifications (nonsmoking, weight reduction, physical activity, and mediterranean diet) after healing of myocardial infarction, percutaneous intervention, or coronary bypass (from the REasons for Geographic and Racial Differences in Stroke Study)
Abstract
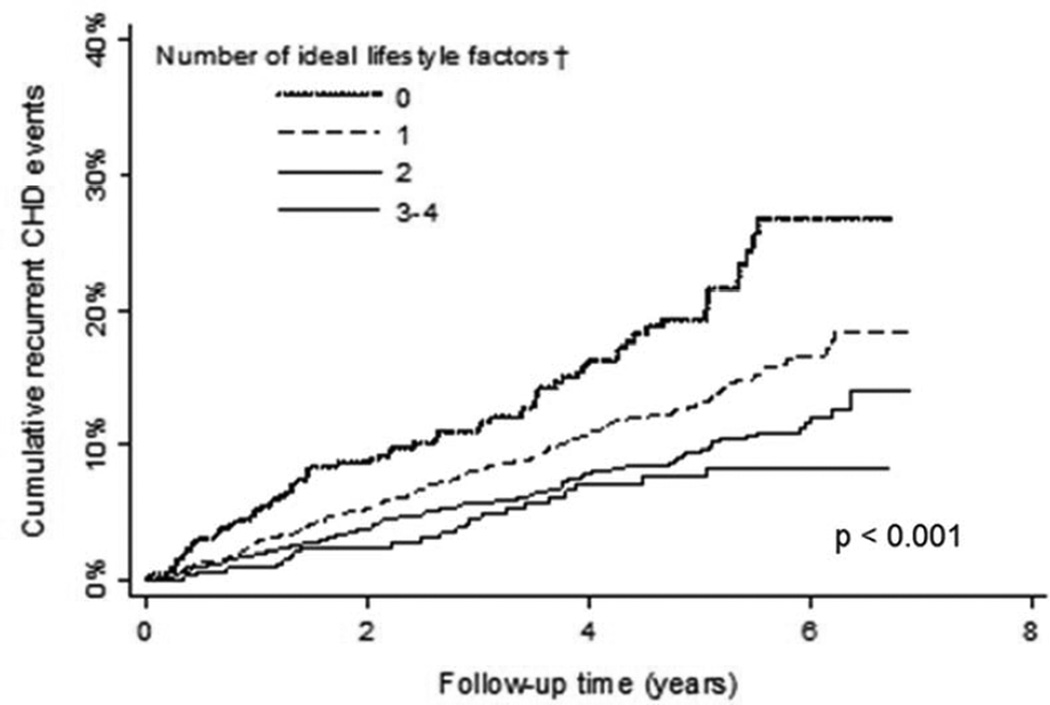
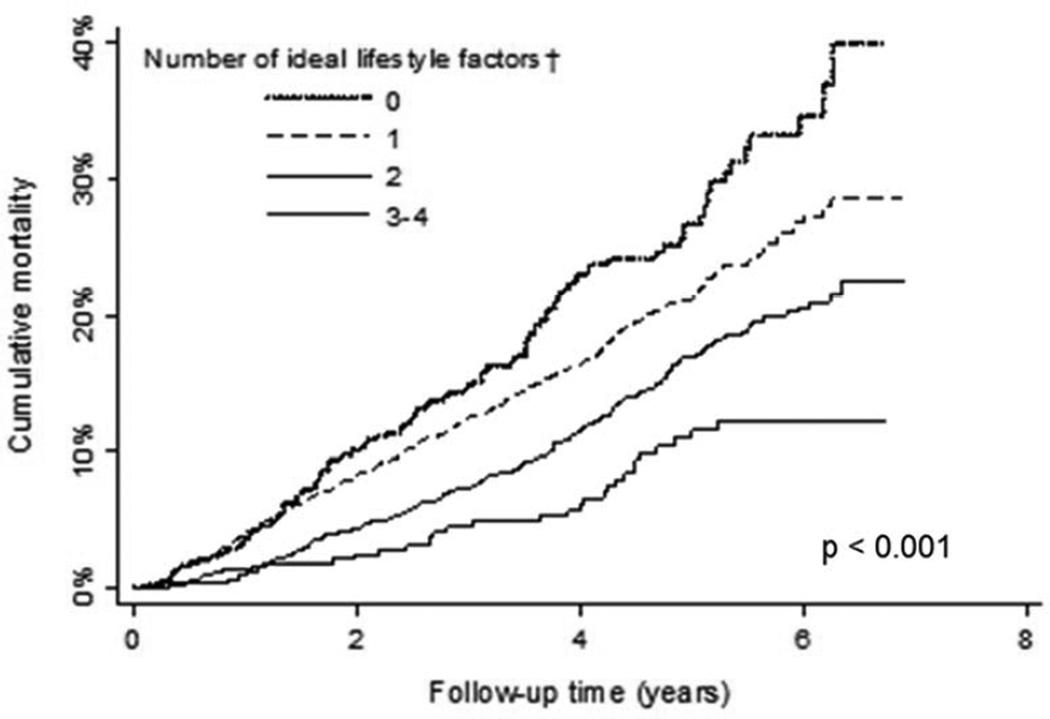
Guidelines recommend lifestyle modification for patients with coronary heart disease (CHD). Few data demonstrate which lifestyle modifications, if sustained, reduce recurrent CHD and mortality risk in cardiac patients after the postacute rehabilitation phase. We determined the association between ideal lifestyle factors and recurrent CHD and all-cause mortality in REasons for Geographic and Racial Differences in Stroke study participants with CHD (n = 4,174). Ideal lifestyle factors (physical activity ≥4 times/week, nonsmoking, highest quartile of Mediterranean diet score, and waist circumference <88 cm for women and <102 cm for men) were assessed through questionnaires and an in-home study visit. There were 447 recurrent CHD events and 745 deaths over a median 4.3 and 4.5 years, respectively. After multivariable adjustment, physical activity ≥4 versus no times/week and non-smoking versus current smoking were associated with reduced hazard ratios (HRs; 95% confidence interval [CI]) for recurrent CHD (HR 0.69, 95% CI 0.54 to 0.89 and HR 0.50, 95% CI 0.39 to 0.64, respectively) and death (HR 0.71, 95% CI 0.59 to 0.86 and HR 0.53, 95% CI 0.44 to 0.65, respectively). The multivariable-adjusted HRs (and 95% CIs) for recurrent CHD and death comparing the highest versus lowest quartile of Mediterranean diet adherence were 0.77 (95% CI 0.55 to 1.06) and 0.84 (95% CI 0.67 to 1.07), respectively. Neither outcome was associated with waist circumference. Comparing participants with 1, 2, and 3 versus 0 ideal lifestyle factors (non-smoking, physical activity ≥4 times/week, and highest quartile of Mediterranean diet score), the HRs (and 95% CIs) were 0.60 (95% CI 0.44 to 0.81), 0.49 (95% CI 0.36 to 0.67), and 0.38 (95% CI 0.21 to 0.67), respectively, for recurrent CHD and 0.65 (95% CI 0.51 to 0.83), 0.57 (95% CI 0.43 to 0.74), and 0.41 (95% CI 0.26 to 0.64), respectively, for death. In conclusion, maintaining smoking cessation, physical activity, and Mediterranean diet adherence is important for secondary CHD prevention.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Dietary Patterns and Mediterranean Diet Score and Hazard of Recurrent Coronary Heart Disease Events and All-Cause Mortality in the REGARDS Study.J Am Heart Assoc. 2018 Jul 12;7(14):e008078. doi: 10.1161/JAHA.117.008078. J Am Heart Assoc. 2018. PMID: 30005552 Free PMC article.
-
Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: the HALE project.JAMA. 2004 Sep 22;292(12):1433-9. doi: 10.1001/jama.292.12.1433. JAMA. 2004. PMID: 15383513
-
Healthy lifestyle factors and incident heart disease and mortality in candidates for primary prevention with statin therapy.Int J Cardiol. 2016 Mar 15;207:196-202. doi: 10.1016/j.ijcard.2016.01.001. Epub 2016 Jan 7. Int J Cardiol. 2016. PMID: 26803243 Free PMC article.
-
Impact of Lifestyle Modifications on Cancer Mortality: A Systematic Review and Meta-Analysis.Medicina (Kaunas). 2025 Feb 10;61(2):307. doi: 10.3390/medicina61020307. Medicina (Kaunas). 2025. PMID: 40005424 Free PMC article.
-
Coronary heart disease risk factors and outcomes in the twenty-first century: findings from the REasons for Geographic and Racial Differences in Stroke (REGARDS) Study.Curr Hypertens Rep. 2015 Apr;17(4):541. doi: 10.1007/s11906-015-0541-5. Curr Hypertens Rep. 2015. PMID: 25794955 Free PMC article. Review.
Cited by
-
Risk Factors and Cardiovascular Disease in the Elderly.Rev Cardiovasc Med. 2022 May 25;23(6):188. doi: 10.31083/j.rcm2306188. eCollection 2022 Jun. Rev Cardiovasc Med. 2022. PMID: 39077174 Free PMC article. Review.
-
A prospective, randomized, controlled, multicentre trial for secondary prevention in patients with chronic coronary syndrome using a smartphone application for digital therapy: the CHANGE study protocol.Eur Heart J Digit Health. 2023 Feb 15;4(3):207-215. doi: 10.1093/ehjdh/ztad012. eCollection 2023 May. Eur Heart J Digit Health. 2023. PMID: 37265862 Free PMC article.
-
Lifestyle Cardiovascular Risk Score, Genetic Risk Score, and Myocardial Infarction in Hispanic/Latino Adults Living in Costa Rica.J Am Heart Assoc. 2016 Dec 20;5(12):e004067. doi: 10.1161/JAHA.116.004067. J Am Heart Assoc. 2016. PMID: 27998913 Free PMC article.
-
Role of High-Sensitivity C-reactive Protein (Hs-CRP) in Non-communicable Diseases: A Review.Cureus. 2022 Oct 12;14(10):e30225. doi: 10.7759/cureus.30225. eCollection 2022 Oct. Cureus. 2022. PMID: 36381804 Free PMC article. Review.
-
Hypothetical model of perceived adherence to treatment among patients with coronary heart disease after a percutaneous coronary intervention.Nurs Open. 2019 Sep 27;7(1):246-255. doi: 10.1002/nop2.381. eCollection 2020 Jan. Nurs Open. 2019. PMID: 31871708 Free PMC article.
References
-
- Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R, Dallongeville J, De Backer G, Ebrahim S, Gjelsvik B, Herrmann-Lingen C, Hoes A, Humphries S, Knapton M, Perk J, Priori SG, Pyorala K, Reiner Z, Ruilope L, Sans-Menendez S, Op Reimer WS, Weissberg P, Wood D, Yarnell J, Zamorano JL, Walma E, Fitzgerald T, Cooney MT, Dudina A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Funck-Brentano C, Filippatos G, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Altiner A, Bonora E, Durrington PN, Fagard R, Giampaoli S, Hemingway H, Hakansson J, Kjeldsen SE, Larsen ML, Mancia G, Manolis AJ, Orth-Gomer K, Pedersen T, Rayner M, Ryden L, Sammut M, Schneiderman N, Stalenhoef AF, Tokgozoglu L, Wiklund O, Zampelas A European Society of C, European Association for Cardiovascular P, Rehabilitation, Council on Cardiovascular N, European Association for Study of D, International Diabetes Federation E, European Stroke I, International Society of Behavioural M, European Society of H, European Society of General Practice/Family M, European Heart N. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts) Eur J Cardiovasc Prev Rehabil. 2007;14(Suppl 2):E1–E40. - PubMed
-
- Smith SC, Jr, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, Gibbons RJ, Grundy SM, Hiratzka LF, Jones DW, Lloyd-Jones DM, Minissian M, Mosca L, Peterson ED, Sacco RL, Spertus J, Stein JH, Taubert KA World Heart F, the Preventive Cardiovascular Nurses A. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;124:2458–2473. - PubMed
-
- Leon AS, Franklin BA, Costa F, Balady GJ, Berra KA, Stewart KJ, Thompson PD, Williams MA, Lauer MS American Heart A, Council on Clinical C, Council on Nutrition PA, Metabolism, American association of C, Pulmonary R. Cardiac rehabilitation and secondary prevention of coronary heart disease: an American Heart Association scientific statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity), in collaboration with the American association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2005;111:369–376. - PubMed
-
- Arena R, Williams M, Forman DE, Cahalin LP, Coke L, Myers J, Hamm L, Kris-Etherton P, Humphrey R, Bittner V, Lavie CJ American Heart Association Exercise CR, Prevention Committee of the Council on Clinical Cardiology CoE, Prevention, Council on Nutrition PA, Metabolism. Increasing referral and participation rates to outpatient cardiac rehabilitation: the valuable role of healthcare professionals in the inpatient and home health settings: a science advisory from the American Heart Association. Circulation. 2012;125:1321–1329. - PubMed
-
- Suaya JA, Shepard DS, Normand SL, Ades PA, Prottas J, Stason WB. Use of cardiac rehabilitation by Medicare beneficiaries after myocardial infarction or coronary bypass surgery. Circulation. 2007;116:1653–1662. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
