

Characterization of a phenotype-based genetic test prediction score for unrelated patients with hypertrophic cardiomyopathy
- PMID: 24793961
- PMCID: PMC4234122
- DOI: 10.1016/j.mayocp.2014.01.025
Characterization of a phenotype-based genetic test prediction score for unrelated patients with hypertrophic cardiomyopathy
Abstract
Objectives: To determine the prevalence and spectrum of mutations and genotype-phenotype relationships in the largest hypertrophic cardiomyopathy (HCM) cohort to date and to provide an easy, clinically applicable phenotype-derived score that provides a pretest probability for a positive HCM genetic test result.
Patients and methods: Between April 1, 1997, and February 1, 2007, 1053 unrelated patients with the clinical diagnosis of HCM (60% male; mean ± SD age at diagnosis, 44.4 ± 19 years) had HCM genetic testing for the 9 HCM-associated myofilament genes. Phenotyping was performed by review of electronic medical records.
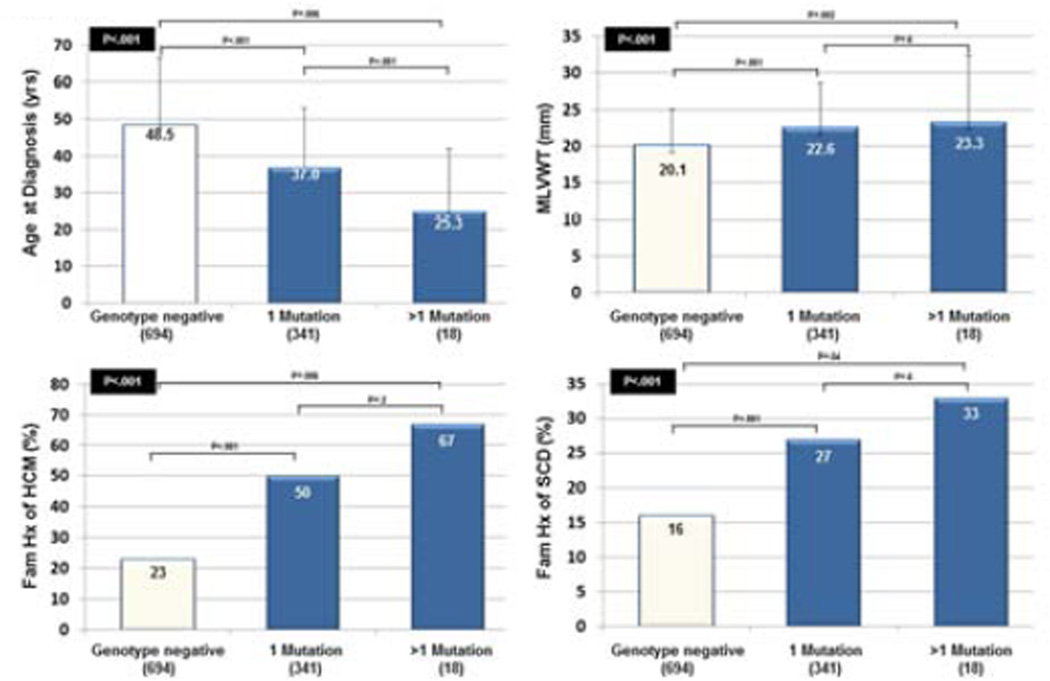
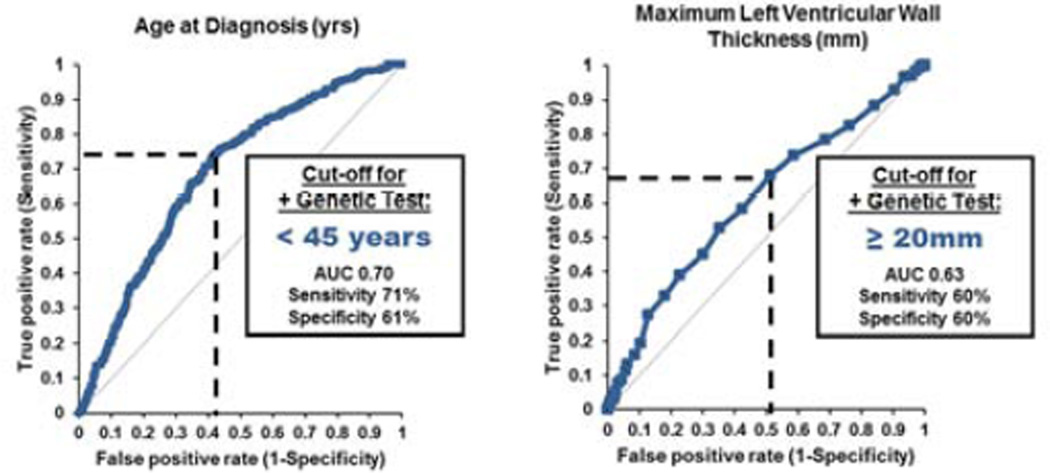
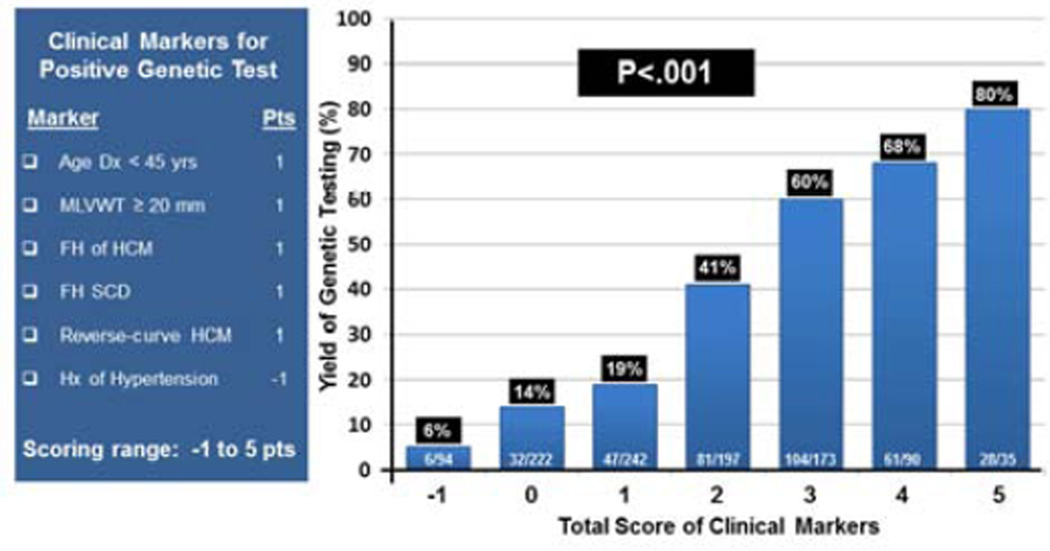
Results: Overall, 359 patients (34%) were genotype positive for a putative HCM-associated mutation in 1 or more HCM-associated genes. Univariate and multivariate analyses identified the echocardiographic reverse curve morphological subtype, an age at diagnosis younger than 45 years, a maximum left ventricular wall thickness of 20 mm or greater, a family history of HCM, and a family history of sudden cardiac death as positive predictors of positive genetic test results, whereas hypertension was a negative predictor. A score, based on the number of predictors of a positive genetic test result, predicted a positive genetic test result ranging from 6% when only hypertension was present to 80% when all 5 positive predictor markers were present.
Conclusion: In this largest HCM cohort published to date, the overall yield of genetic testing was 34%. Although all the patients were diagnosed clinically as having HCM, the presence or absence of 6 simple clinical/echocardiographic markers predicted the likelihood of mutation-positive HCM. Phenotype-guided genetic testing using the Mayo HCM Genotype Predictor score provides an easy tool for an effective genetic counseling session.
Copyright © 2014 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
MJA is a consultant for Boston Scientific, Medtronic, St. Jude Medical, Inc., and Transgenomic. Intellectual property derived from MJA’s research program resulted in license agreements in 2004 between Mayo Clinic Health Solutions (formerly Mayo Medical Ventures) and PGxHealth (formerly Genaissance Pharmaceuticals, now Transgenomic) with respect to their FAMILION-LQTS and FAMILION-CPVT genetic tests but not their FAMILION-HCM genetic test. The other authors have no conflicts of interest to disclose. None of the disclosures pertain to this study and none of the companies provided financial support for this study.
Figures
References
-
- Maron BJ. Hypertrophic cardiomyopathy: A systematic review. JAMA. 2002;287(10):1308–1320. - PubMed
-
- Maron B, Epstein S, Roberts W. Causes of sudden death in competitive athletes. J Am Coll Cardiol. 1986;7(1):204–214. - PubMed
-
- Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden Deaths in Young Competitive Athletes: Analysis of 1866 Deaths in the United States, 1980- 2006. Circulation. 2009;119(8):1085–1092. - PubMed
-
- Ackerman MJ, Priori SG, Willems S, et al. HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies this document was developed as a partnership between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA) Heart Rhythm. 2011;8(8):1308–1339. - PubMed
-
- Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;58(25):e212–e260. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
