

Effect of fluconazole prophylaxis on candidiasis and mortality in premature infants: a randomized clinical trial
- PMID: 24794367
- PMCID: PMC4110724
- DOI: 10.1001/jama.2014.2624
Effect of fluconazole prophylaxis on candidiasis and mortality in premature infants: a randomized clinical trial
Abstract
Importance: Invasive candidiasis in premature infants causes death and neurodevelopmental impairment. Fluconazole prophylaxis reduces candidiasis, but its effect on mortality and the safety of fluconazole are unknown.
Objective: To evaluate the efficacy and safety of fluconazole in preventing death or invasive candidiasis in extremely low-birth-weight infants.
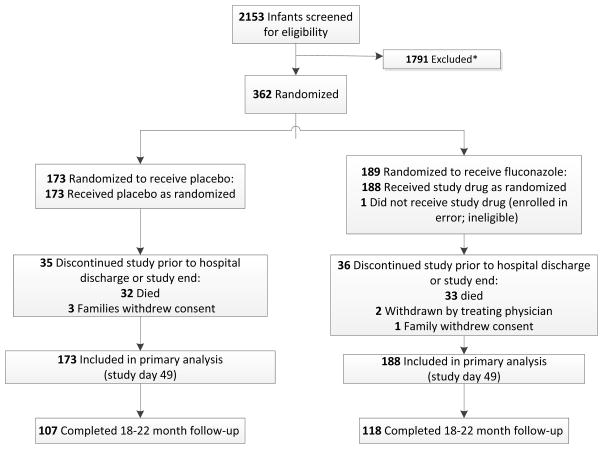
Design, setting, and patients: This study was a randomized, blinded, placebo-controlled trial of fluconazole in premature infants. Infants weighing less than 750 g at birth (N = 361) from 32 neonatal intensive care units (NICUs) in the United States were randomly assigned to receive either fluconazole or placebo twice weekly for 42 days. Surviving infants were evaluated at 18 to 22 months corrected age for neurodevelopmental outcomes. The study was conducted between November 2008 and February 2013.
Interventions: Fluconazole (6 mg/kg of body weight) or placebo.
Main outcomes and measures: The primary end point was a composite of death or definite or probable invasive candidiasis prior to study day 49 (1 week after completion of study drug). Secondary and safety outcomes included invasive candidiasis, liver function, bacterial infection, length of stay, intracranial hemorrhage, periventricular leukomalacia, chronic lung disease, patent ductus arteriosus requiring surgery, retinopathy of prematurity requiring surgery, necrotizing enterocolitis, spontaneous intestinal perforation, and neurodevelopmental outcomes-defined as a Bayley-III cognition composite score of less than 70, blindness, deafness, or cerebral palsy at 18 to 22 months corrected age.
Results: Among infants receiving fluconazole, the composite primary end point of death or invasive candidiasis was 16% (95% CI, 11%-22%) vs 21% in the placebo group (95% CI, 15%-28%; odds ratio, 0.73 [95% CI, 0.43-1.23]; P = .24; treatment difference, -5% [95% CI, -13% to 3%]). Invasive candidiasis occurred less frequently in the fluconazole group (3% [95% CI, 1%-6%]) vs the placebo group (9% [95% CI, 5%-14%]; P = .02; treatment difference, -6% [95% CI, -11% to -1%]). The cumulative incidences of other secondary outcomes were not statistically different between groups. Neurodevelopmental impairment did not differ between the groups (fluconazole, 31% [95% CI, 21%-41%] vs placebo, 27% [95% CI, 18%-37%]; P = .60; treatment difference, 4% [95% CI, -10% to 17%]).
Conclusions and relevance: Among infants with a birth weight of less than 750 g, 42 days of fluconazole prophylaxis compared with placebo did not result in a lower incidence of the composite of death or invasive candidiasis. These findings do not support the universal use of prophylactic fluconazole in extremely low-birth-weight infants.
Trial registration: clinicaltrials.gov Identifier: NCT00734539.
Conflict of interest statement
All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Benjamin reports receipt of support from the National Institutes of Health (NIH), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the US Food and Drug Administration (USFDA), and the National Center for Advancing Translational Sciences of the NIH for work in pediatric and neonatal clinical pharmacology, and the nonprofit organization Thrasher Research Fund for work in neonatal candidiasis; and research support from industry for neonatal and pediatric drug development (
Figures
Comment in
-
[Prophylaxis with fluconazole on invasive candidiasis and mortality in premature infants].Rev Chilena Infectol. 2014 Aug;31(4):488. doi: 10.4067/S0716-10182014000400020. Rev Chilena Infectol. 2014. PMID: 25327208 Spanish. No abstract available.
-
Fluconazole prophylaxis in neonates.Arch Dis Child. 2015 Jan;100(1):75-6. doi: 10.1136/archdischild-2014-306771. Epub 2014 Oct 23. Arch Dis Child. 2015. PMID: 25341552 No abstract available.
-
Does fluconazole prophylaxis reduce death or invasive candida infection in extremely preterm infants?Acta Paediatr. 2017 May;106(5):844-845. doi: 10.1111/apa.13719. Epub 2017 Jan 25. Acta Paediatr. 2017. PMID: 28120400 Free PMC article. No abstract available.
References
-
- Stoll BJ, Hansen N, Fanaroff AA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics. 2002;110(2 Pt 1):285–291. - PubMed
-
- Benjamin DK, Jr, Stoll BJ, Fanaroff AA, et al. Neonatal candidiasis among extremely low birth weight infants: risk factors, mortality, and neurodevelopmental outcomes at 18–22 months. Pediatrics. 2006;117(1):84–92. - PubMed
-
- Manzoni P, Stolfi I, Pugni L, et al. A multicenter, randomized trial of prophylactic fluconazole in preterm neonates. N Engl J Med. 2007;356(24):2483–2495. - PubMed
-
- Kaufman D, Boyle R, Hazen KC, Patrie JT, Robinson M, Donowitz LG. Fluconazole prophylaxis against fungal colonization and infection in preterm infants. N Engl J Med. 2001;345(23):1660–1666. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
