

Safety and immunogenicity of tetanus diphtheria and acellular pertussis (Tdap) immunization during pregnancy in mothers and infants: a randomized clinical trial
- PMID: 24794369
- PMCID: PMC4333147
- DOI: 10.1001/jama.2014.3633
Safety and immunogenicity of tetanus diphtheria and acellular pertussis (Tdap) immunization during pregnancy in mothers and infants: a randomized clinical trial
Erratum in
-
Data Errors in Table.JAMA. 2017 Jan 24;317(4):442. doi: 10.1001/jama.2016.20705. JAMA. 2017. PMID: 28118432 No abstract available.
-
Notice of Data Errors.JAMA. 2017 Jan 24;317(4):441-442. doi: 10.1001/jama.2016.19244. JAMA. 2017. PMID: 28118445 No abstract available.
Abstract
Importance: Maternal immunization with tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine could prevent infant pertussis.
Objective: To evaluate the safety and immunogenicity of Tdap immunization during pregnancy and its effect on infant responses to diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccine.
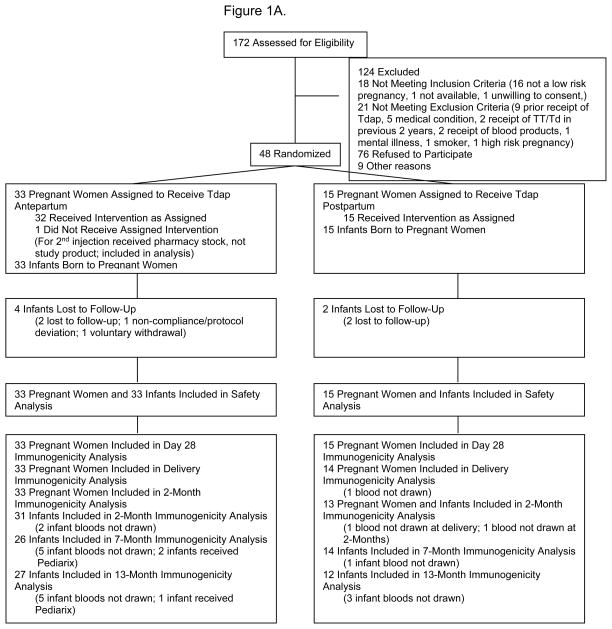
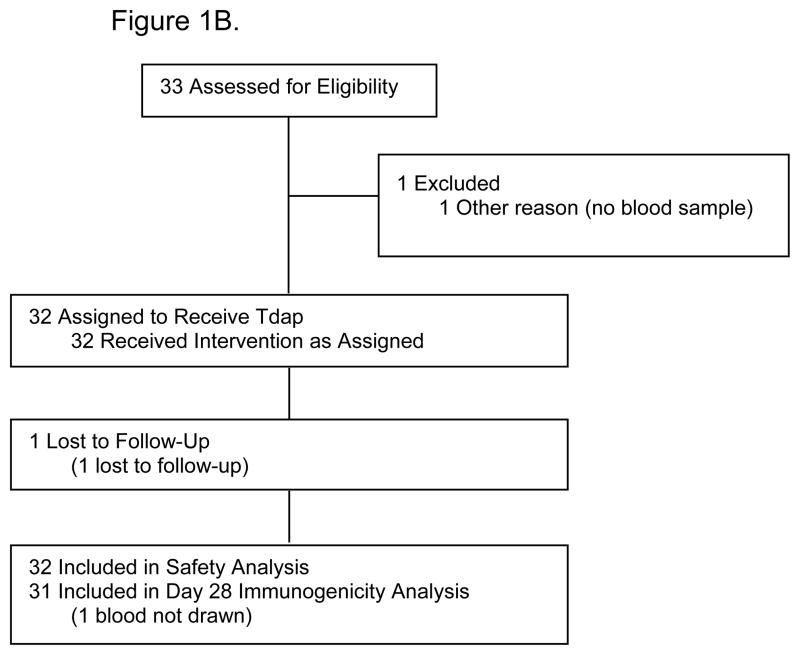
Design, setting, and participants: Phase 1-2, randomized, double-blind, placebo-controlled, clinical trial conducted from 2008 to 2012. Forty-eight pregnant women aged 18 to 45 years received Tdap (n = 33) or placebo (n = 15) at 30 to 32 weeks' gestation, with crossover immunization postpartum.
Interventions: Tdap vaccination at 30 to 32 weeks' gestation or postpartum.
Main outcomes and measures: Primary outcomes were maternal and infant adverse events, pertussis illness, and infant growth and development until age 13 months. Secondary outcomes were antibody concentrations in pregnant women before and 4 weeks after Tdap immunization or placebo, at delivery and 2 months' postpartum, and in infants at birth, at 2 months, and after the third and fourth doses of DTaP.
Results: No Tdap-associated serious adverse events occurred in women or infants. Injection site reactions after Tdap immunization were reported in 26 (78.8% [95% CI, 61.1%-91.0%]) and 12 (80% [95% CI, 51.9%-95.7%]) pregnant and postpartum women, respectively (P > .99). Systemic symptoms were reported in 12 (36.4% [ 95% CI, 20.4%-54.9%]) and 11 (73.3% [95% CI, 44.9%-92.2%]) pregnant and postpartum women, respectively (P = .03). Growth and development were similar in both infant groups. No cases of pertussis occurred. Significantly higher concentrations of pertussis antibodies were measured at delivery in women who received Tdap during pregnancy vs postpartum (eg, pertussis toxin antibodies: 51.0 EU/mL [95% CI, 37.1-70.1] and 9.1 EU/mL [95% CI, 4.6-17.8], respectively; P < .001) and in their infants at birth (68.8 EU/mL [95% CI, 52.1-90.8] and 14.0 EU/mL [95% CI, 7.3-26.9], respectively; P < .001) and at age 2 months (20.6 EU/mL [95% CI, 14.4-29.6] and 5.3 EU/mL [95% CI, 3.0-9.4], respectively; P < .001). Antibody responses in infants born to women receiving Tdap during pregnancy were not different following the fourth dose of DTaP.
Conclusions and relevance: This preliminary assessment did not find an increased risk of adverse events among women who received Tdap vaccine during pregnancy or their infants. For secondary outcomes, maternal immunization with Tdap resulted in high concentrations of pertussis antibodies in infants during the first 2 months of life and did not substantially alter infant responses to DTaP. Further research is needed to provide definitive evidence of the safety and efficacy of Tdap immunization during pregnancy.
Trial registration: clinicaltrials.gov Identifier: NCT00707148.
Conflict of interest statement
Conflict of Interest:
No conflict of interest related to this study was reported by the following authors: Bond, Maccato, Pinell, Hammill, Jackson, C. R. Petrie, J. Ferreira and J. Goll performed this work supported by NIAID-DMID contract (Clinical Research in Infectious Disease (CRID), HHSN272200800013C).
F. Munoz has served as a speaker for Sanofi Pasteur and as consultant for Novartis, GlaxoSmithKline (GSK), and Novavax. She has also conducted clinical trials sponsored by Hoffmann-LaRoche, GlaxoSmithKline Biologicals, and Gilead Sciences.
G. Swamy reports receiving consulting and lecturing fees as well as grant support for vaccine-related studies from GSK, as well as for advisory boards, lectures, and the development of educational presentations. She has received grant funding from GSK specific to influenza vaccine and HPV infection.
E. Walter has served as a consultant and advisor for Merck and as a speaker for Sanofi Pasteur. He has conducted clinical trials sponsored by GSK, Merck, Novartis, and Pfizer.
J. Englund has received research support from Novartis, Gilead, Chimerix, and Roche. She was a consultant for GSK in 2012–2013 and served on a GSK DSMB on 2012–13, she also received travel expenses from Abbvie (part of Abbot) in 2013.
M. Edwards serves as consultant for and has received grants from Novartis Vaccines.
C. Healy has conducted trials with grants from Sanofi Pasteur and Novartis, and serves as advisor for Novartis Vaccines..
C. Baker serves as consultant and advisory board member to Novartis Vaccines, and advisory board member for Pfizer Inc.
Figures
Comment in
-
Maternal pertussis immunization: can it help infants?JAMA. 2014 May 7;311(17):1736-7. doi: 10.1001/jama.2014.3555. JAMA. 2014. PMID: 24794364 No abstract available.
-
TDM Journal Club: Safety and Immunogenicity of Tetanus Diphtheria and Acellular Pertussis Immunization During Pregnancy.Ther Drug Monit. 2015 Jun;37(3):283-4. doi: 10.1097/FTD.0000000000000143. Ther Drug Monit. 2015. PMID: 25271727 No abstract available.
References
-
- Vitek CR, Pascual FB, Baughman AL, Murphy TL. Increase in deaths from pertussis among young infants in the United States in the 1990s. Pediatr Infect Dis J. 2003 Jul;22(7):628–34. - PubMed
-
- Healy CM, Munoz FM, Rench MA, Halasa NB, Edwards KM, Baker CJ. Prevalence of pertussis antibodies in maternal delivery, cord, and infant serum. J Infect Dis. 2004;190:335–40. - PubMed
-
- Van Savage J, Decker MD, Edwards KM, Sell SH, Karzon DT. Natural history of pertussis antibody in the infant and effect on vaccine response. J Infect Dis. 1990;161:487–92. - PubMed
-
- Centers for Disease Control and Prevention, Advisory Committee on Immunization Practices (ACIP) Preventing tetanus, diphtheria, and pertussis among adolescents: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines, recommendations of the ACIP. MMWR Recomm Rep. 2006 Mar 24;55(RR-3):1–34. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
