

Axitinib sensitization of high Single Dose Radiotherapy
- PMID: 24794795
- PMCID: PMC4278650
- DOI: 10.1016/j.radonc.2014.02.010
Axitinib sensitization of high Single Dose Radiotherapy
Abstract
Background and purpose: Single Dose Radiation Therapy (SDRT) provides remarkably high rates of control even for tumors resistant to fractionated radiotherapy. SDRT tumor control depends on acute acid sphingomyelinase-mediated endothelial cell injury and monoclonal antibodies targeting Vascular Endothelial Cell Growth Factor (VEGF) signaling radiosensitized tumor endothelium when delivered immediately prior to irradiation. Here we evaluate the ability of the oral VEGF receptor inhibitor, axitinib, to sensitize tumor endothelium and increase tumor control with SDRT.
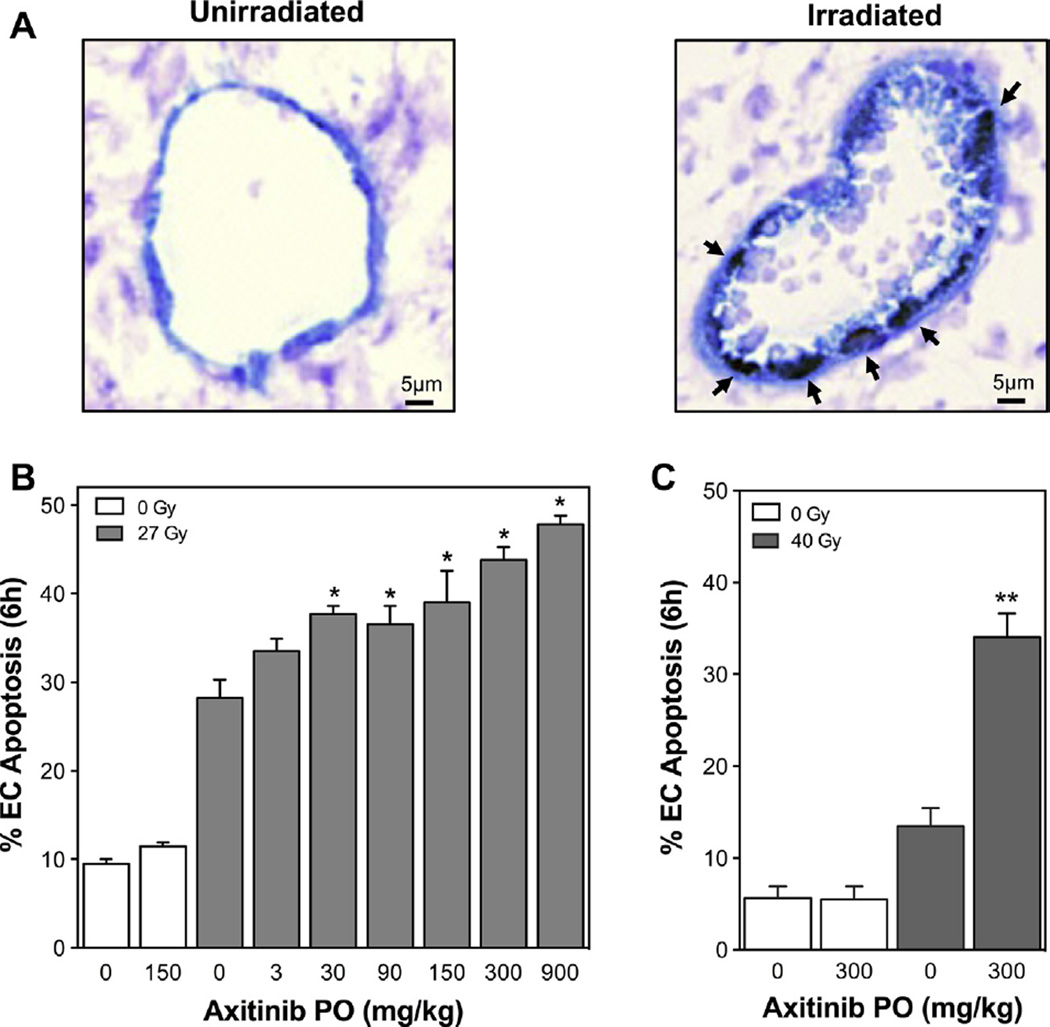
Methods and materials: Axitinib was added to primary cultured endothelial cells, or administered orally to Sv129/BL6 mice bearing radiosensitive MCA/129 sarcoma or radioresistant B16F1 melanoma flank tumors, followed by SDRT. Endothelial apoptosis was assessed by TUNEL assay or bis-benzamide staining. Mice with irradiated tumors were followed for 90days to evaluate the impact of axitinib on SDRT tumor control.
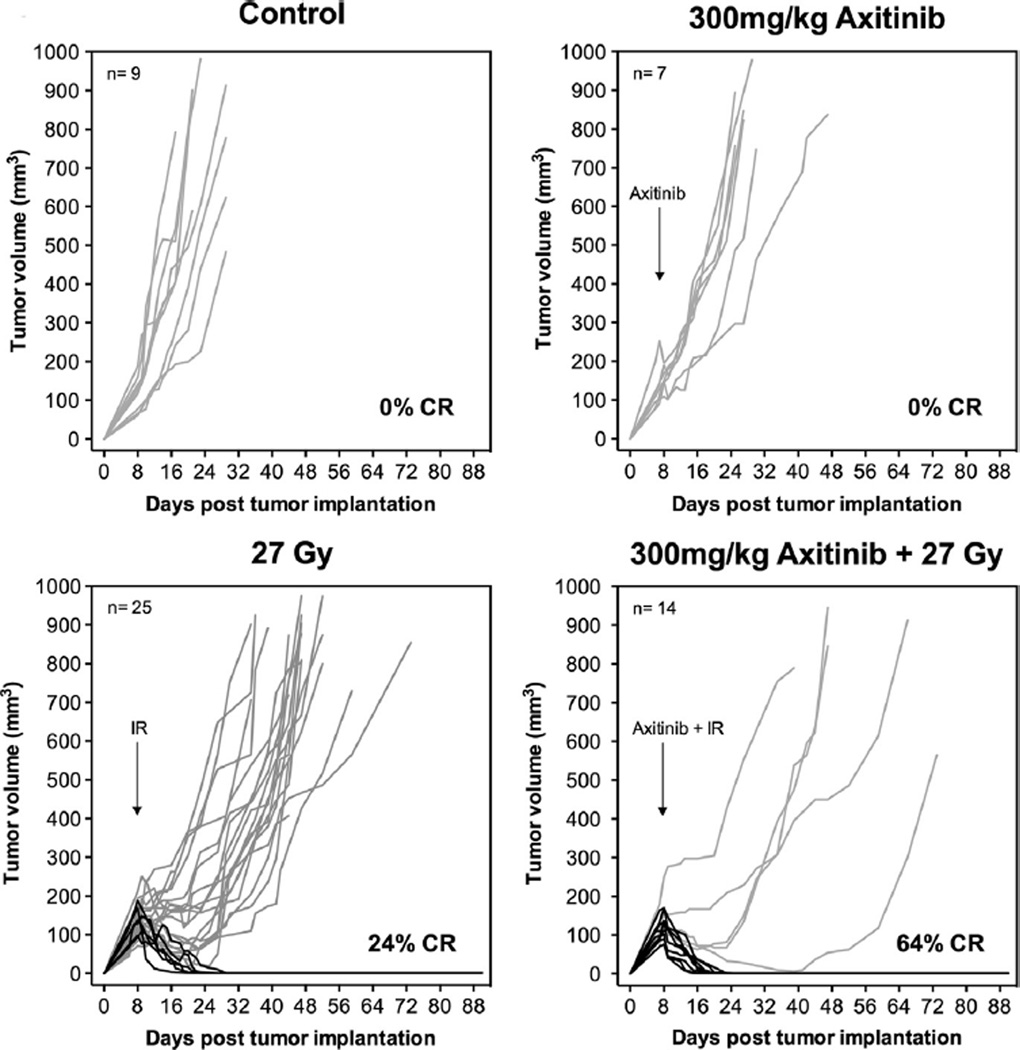
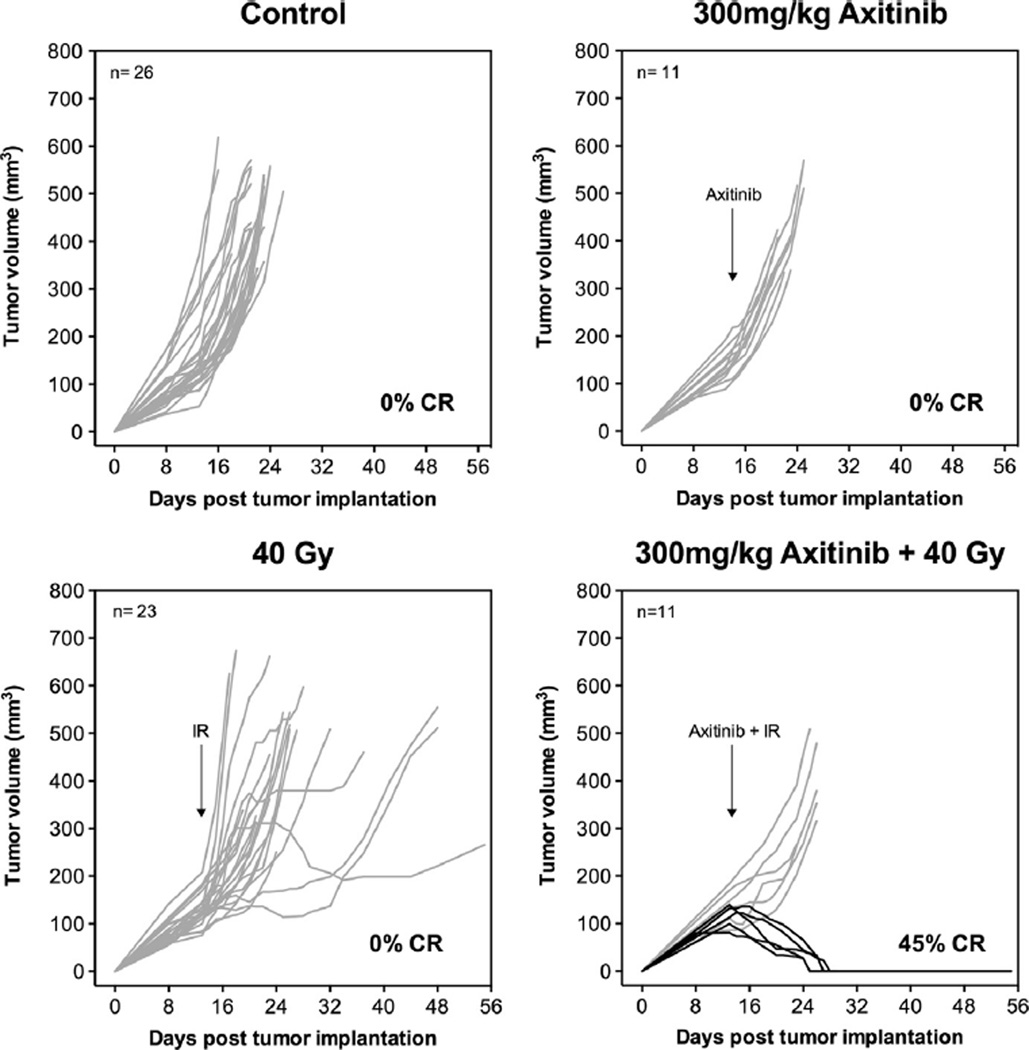
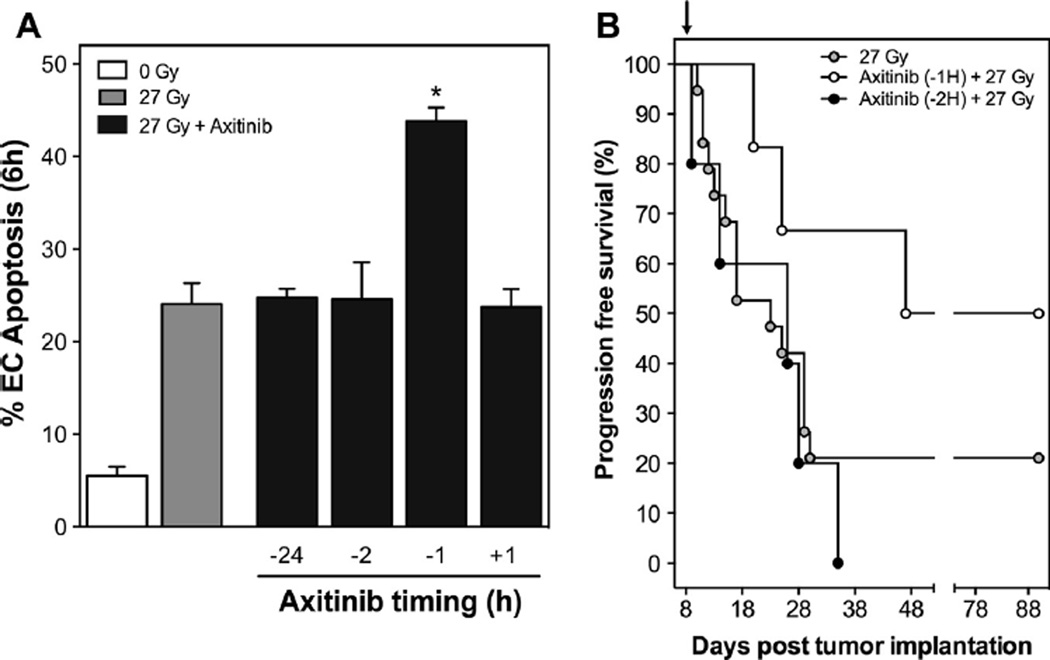
Results: Pre-treatment with axitinib increased acute endothelial cell apoptosis following SDRT in vitro, and in vivo for both MCA/129 and B16F1 tumors. Axitinib correspondingly increased SDRT tumor growth delay and complete response rate (by 40%) for both tumors. Administration precisely 1h before SDRT was critical for radiosensitization.
Conclusions: Axitinib radiosensitizes tumor endothelial cells and enhances tumor cure with SDRT, which may permit dose de-escalation and significantly expand the range of clinical indications for SDRT.
Keywords: Acid sphingomyelinase; Anti-angiogenic; Ceramide; Radiosurgery; Stereotactic body radiation therapy; Vascular endothelial growth factor.
Copyright © 2014. Published by Elsevier Ireland Ltd.
Conflict of interest statement
None.
Figures
Similar articles
-
Endothelial membrane remodeling is obligate for anti-angiogenic radiosensitization during tumor radiosurgery.PLoS One. 2010 Aug 19;5(8):e12310. doi: 10.1371/journal.pone.0012310. PLoS One. 2010. PMID: 20808818 Free PMC article.
-
Adenoviral transduction of human acid sphingomyelinase into neo-angiogenic endothelium radiosensitizes tumor cure.PLoS One. 2013 Aug 2;8(8):e69025. doi: 10.1371/journal.pone.0069025. Print 2013. PLoS One. 2013. PMID: 23936314 Free PMC article.
-
Nonclinical antiangiogenesis and antitumor activities of axitinib (AG-013736), an oral, potent, and selective inhibitor of vascular endothelial growth factor receptor tyrosine kinases 1, 2, 3.Clin Cancer Res. 2008 Nov 15;14(22):7272-83. doi: 10.1158/1078-0432.CCR-08-0652. Clin Cancer Res. 2008. PMID: 19010843
-
Axitinib in metastatic renal cell carcinoma.Expert Rev Anticancer Ther. 2015 May;15(5):499-507. doi: 10.1586/14737140.2015.1033408. Expert Rev Anticancer Ther. 2015. PMID: 25907705 Review.
-
Axitinib: from preclinical development to future clinical perspectives in renal cell carcinoma.Expert Opin Drug Discov. 2015;10(8):925-35. doi: 10.1517/17460441.2015.1045411. Epub 2015 Jun 3. Expert Opin Drug Discov. 2015. PMID: 26039031 Review.
Cited by
-
Small Molecule Inhibitors for Hepatocellular Carcinoma: Advances and Challenges.Molecules. 2022 Aug 28;27(17):5537. doi: 10.3390/molecules27175537. Molecules. 2022. PMID: 36080304 Free PMC article. Review.
-
Single-dose radiotherapy disables tumor cell homologous recombination via ischemia/reperfusion injury.J Clin Invest. 2019 Feb 1;129(2):786-801. doi: 10.1172/JCI97631. Epub 2019 Jan 14. J Clin Invest. 2019. PMID: 30480549 Free PMC article.
-
The importance of multidisciplinary care for spine metastases: initial tumor management.Neurooncol Pract. 2020 Nov 18;7(Suppl 1):i25-i32. doi: 10.1093/nop/npaa056. eCollection 2020 Nov. Neurooncol Pract. 2020. PMID: 33299571 Free PMC article. Review.
-
Impacts of Ionizing Radiation on the Different Compartments of the Tumor Microenvironment.Front Pharmacol. 2016 Mar 30;7:78. doi: 10.3389/fphar.2016.00078. eCollection 2016. Front Pharmacol. 2016. PMID: 27064581 Free PMC article. Review.
-
Molecular Mechanisms of Radiation-Induced Cancer Cell Death: A Primer.Front Cell Dev Biol. 2020 Feb 13;8:41. doi: 10.3389/fcell.2020.00041. eCollection 2020. Front Cell Dev Biol. 2020. PMID: 32117972 Free PMC article. Review.
References
-
- Budach W, et al. Impact of stromal sensitivity on radiation response of tumors. J Natl Cancer Inst. 1993;85:988–993. - PubMed
-
- Gerweck LE, et al. Tumor cell radiosensitivity is a major determinant of tumor response to radiation. Cancer Res. 2006;66:8352–8355. - PubMed
-
- Ogawa K, et al. Influence of tumor cell and stroma sensitivity on tumor response to radiation. Cancer Res. 2007;67:4016–4021. - PubMed
-
- Garcia-Barros M, et al. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science. 2003;300:1155–1159. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
