

Anti-adhesion barrier gels following operative hysteroscopy for treating female infertility: a systematic review and meta-analysis
- PMID: 24795547
- PMCID: PMC4003345
- DOI: 10.1007/s10397-014-0832-x
Anti-adhesion barrier gels following operative hysteroscopy for treating female infertility: a systematic review and meta-analysis
Abstract
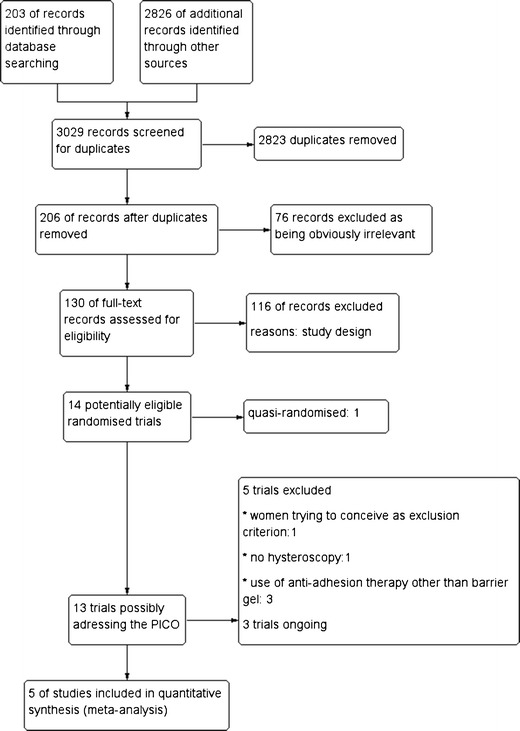
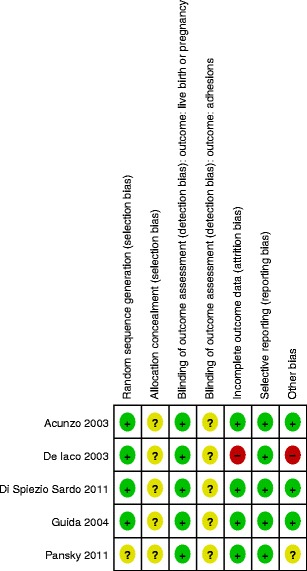
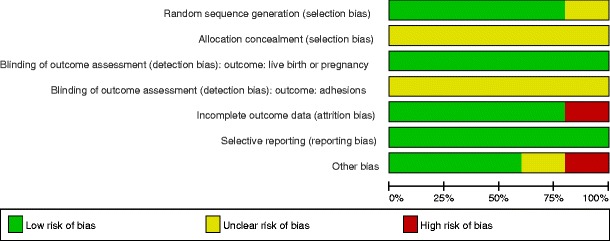
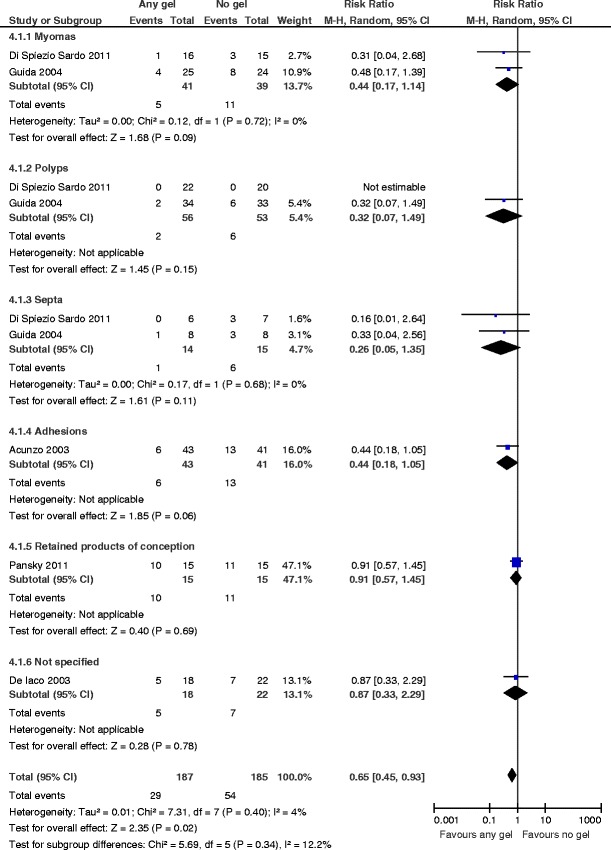
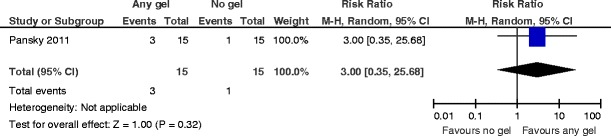
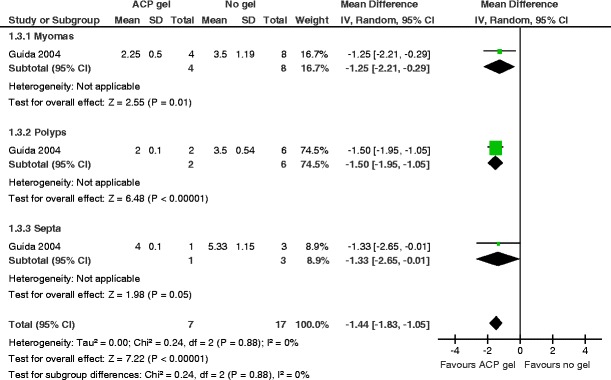
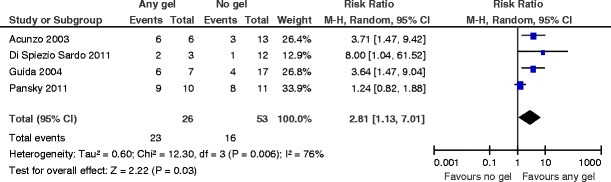
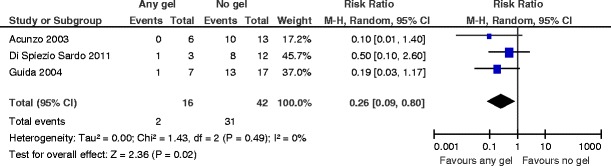
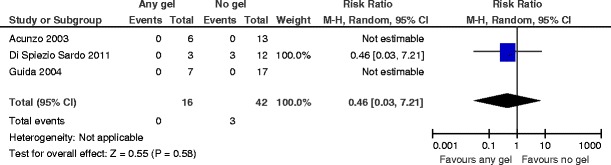
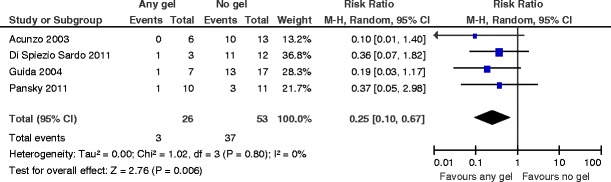
The aim of this study was to assess the effects of any anti-adhesion barrier gel used after operative hysteroscopy for treating infertility associated with uterine cavity abnormalities. Gynecologists might use any barrier gel following operative hysteroscopy in infertile women for decreasing de novo adhesion formation; the use of any barrier gel is associated with less severe de novo adhesions and lower mean adhesion scores. Nevertheless, infertile women should be counseled that there is at the present no evidence for higher live birth or pregnancy rates. There is a lack of data for the outcome miscarriage. Preclinical studies suggest that the use of biodegradable surgical barriers may decrease postsurgical adhesion formation. Observational studies in the human report conflicting results. We searched the Cochrane Menstrual Disorders and Subfertility Specialized Register (10 April 2013), the Cochrane Central Register of Controlled Trials (The Cochrane Library 2013, Issue 1), MEDLINE (1950 to 4 April 2013), EMBASE (1974 to 4 April 2013), and other electronic databases of trials including trial registers, sources of unpublished literature, and reference lists. We handsearched the Journal of Minimally Invasive Gynecology (from 1 January 1992 to 13 April 2013); we also contacted experts in the field. We included the randomized comparisons between any anti-adhesion barrier gel versus another barrier gel, placebo, or no adjunctive therapy following operative hysteroscopy. Primary outcomes were live birth rates and de novo adhesion formation at second-look hysteroscopy. Secondary outcomes were pregnancy and miscarriage rates, mean adhesion scores, and severity of adhesions at second-look hysteroscopy. Two authors independently assessed eligible studies for inclusion and risk of bias, and extracted data. We contacted primary study authors for additional information or other clarification. Five trials met the inclusion criteria. There is no evidence for an effect favoring the use of any barrier gel following operative hysteroscopy for the key outcomes of live birth or clinical pregnancy (risk ratio (RR) 3.0, 95 % confidence interval (CI) 0.35 to 26, P = 0.32, one study, 30 women, very low quality evidence); there were no data on the outcome miscarriage. The use of any gel following operative hysteroscopy decreases the incidence of de novo adhesions at second-look hysteroscopy at 1 to 3 months (RR 0.65, 95 % CI 0.45 to 0.93, P = 0.02, five studies, 372 women, very low quality evidence). The number needed to treat to benefit is 9 (95 % CI 5 to 33). The use of auto-cross-linked hyaluronic acid gel in women undergoing operative hysteroscopy for fibroids, endometrial polyps, or uterine septa is associated with a lower mean adhesion score at second-look hysteroscopy at 3 months (mean difference (MD) -1.44, 95 % CI -1.83 to -1.05, P < 0.00001, one study, 24 women; this benefit is even larger in women undergoing operative hysteroscopy for intrauterine adhesions(MD -3.30, 95 % CI -3.43 to -3.17, P < 0.00001, one study, 19 women). After using any gel following operative hysteroscopy, there are more American Fertility Society 1988 stage I (mild) adhesions (RR 2.81, 95 % CI 1.13 to 7.01, P = 0.03, four studies, 79 women). The number needed to treat to benefit is 2 (95 % CI 1 to 4). Similarly there are less' moderate or severe adhesions' at second-look hysteroscopy (RR 0.25, 95 % CI 0.10 to 0.67, P = 0.006, four studies, 79 women). The number needed to treat to benefit is 2 (95 % CI 1 to 4) (all very low quality evidence). There are some concerns for the non-methodological quality. Only two trials included infertile women; in the remaining three studies, it is not clear whether and how many participants suffered from infertility. Therefore, the applicability of the findings of the included studies to the target population under study should be questioned. Moreover, only one small trial studied the effects of anti-adhesion barrier gels for the key outcome of pregnancy; the length of follow-up was, however, not specified. More well-designed and adequately powered randomized studies are needed to assess whether the use of any anti-adhesion gel affects the key reproductive outcomes in a target population of infertile women.
Keywords: Adhesion prevention; Barrier gel; Infertility; Meta-analysis; Operative hysteroscopy; Systematic review.
Figures

Similar articles
-
Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities.Cochrane Database Syst Rev. 2018 Dec 5;12(12):CD009461. doi: 10.1002/14651858.CD009461.pub4. Cochrane Database Syst Rev. 2018. PMID: 30521679 Free PMC article.
-
Barrier agents for adhesion prevention after gynaecological surgery.Cochrane Database Syst Rev. 2020 Mar 22;3(3):CD000475. doi: 10.1002/14651858.CD000475.pub4. Cochrane Database Syst Rev. 2020. PMID: 32199406 Free PMC article.
-
Fluid and pharmacological agents for adhesion prevention after gynaecological surgery.Cochrane Database Syst Rev. 2020 Jul 17;7(7):CD001298. doi: 10.1002/14651858.CD001298.pub5. Cochrane Database Syst Rev. 2020. PMID: 32683695 Free PMC article.
-
Anti-adhesion Gel versus No gel following Operative Hysteroscopy prior to Subsequent fertility Treatment or timed InterCourse (AGNOHSTIC), a randomised controlled trial: protocol.Hum Reprod Open. 2021 Feb 16;2021(1):hoab001. doi: 10.1093/hropen/hoab001. eCollection 2021. Hum Reprod Open. 2021. PMID: 33623830 Free PMC article. Review.
-
Efficacy of Hysteroscopy in Improving Fertility Outcomes in Women Undergoing Assisted Reproductive Technique: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Gynecol Obstet Invest. 2023;88(6):336-348. doi: 10.1159/000534794. Epub 2023 Oct 27. Gynecol Obstet Invest. 2023. PMID: 37899034 Free PMC article.
Cited by
-
Safety of menstrual blood-derived stromal cell transplantation in treatment of intrauterine adhesion.World J Stem Cells. 2020 May 26;12(5):368-380. doi: 10.4252/wjsc.v12.i5.368. World J Stem Cells. 2020. PMID: 32547685 Free PMC article.
-
Recent Advances in Understandings Towards Pathogenesis and Treatment for Intrauterine Adhesion and Disruptive Insights from Single-Cell Analysis.Reprod Sci. 2021 Jul;28(7):1812-1826. doi: 10.1007/s43032-020-00343-y. Epub 2020 Oct 30. Reprod Sci. 2021. PMID: 33125685 Free PMC article. Review.
-
Ultrasound evaluation of changes in endometrial receptivity from the day of ovulation to the day of transfer in patients with a history of intrauterine adhesions: a prospective cohort study.Quant Imaging Med Surg. 2025 May 1;15(5):4541-4556. doi: 10.21037/qims-24-2034. Epub 2025 Apr 16. Quant Imaging Med Surg. 2025. PMID: 40384661 Free PMC article.
-
Randomized Controlled Trial of Hyalobarrier® Versus No Hyalobarrier® on the Ovulatory Status of Women with Periovarian Adhesions: A Pilot Study.Adv Ther. 2017 Jan;34(1):199-206. doi: 10.1007/s12325-016-0453-z. Epub 2016 Nov 29. Adv Ther. 2017. PMID: 27900662 Free PMC article. Clinical Trial.
-
Preliminary design of a new degradable medical device to prevent the formation and recurrence of intrauterine adhesions.Commun Biol. 2019 May 22;2:196. doi: 10.1038/s42003-019-0447-x. eCollection 2019. Commun Biol. 2019. PMID: 31123719 Free PMC article.
References
-
- Okulicz WC. Regeneration. In: Glasser SR, Aplin JD, Giudice LC, Tabibzadeh S, editors. The endometrium. London: Taylor and Francis; 2002. pp. 110–120.
-
- Schenker JG, Margalioth EJ. Intrauterine adhesions: an updated appraisal. Fertil Steril. 1982;37:593–610. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous