

Positron emission tomography imaging for vascular inflammation evaluation in elderly subjects with different risk factors for cardiovascular diseases
- PMID: 24795842
- PMCID: PMC3999408
Positron emission tomography imaging for vascular inflammation evaluation in elderly subjects with different risk factors for cardiovascular diseases
Abstract
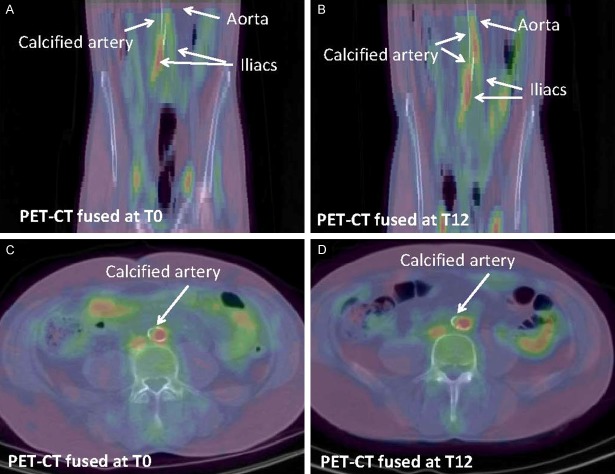
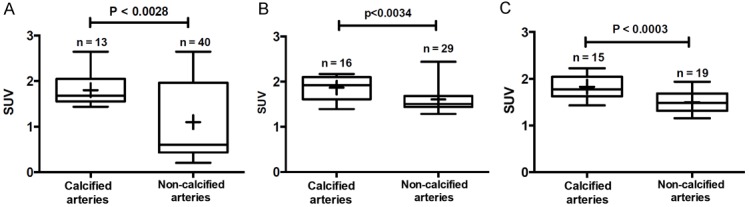
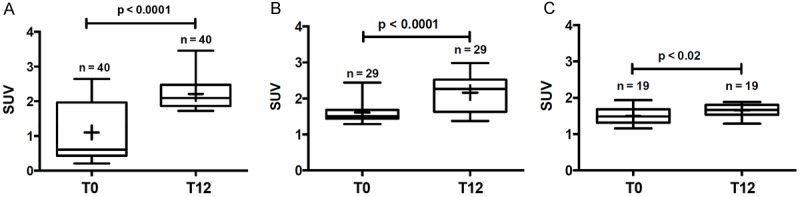
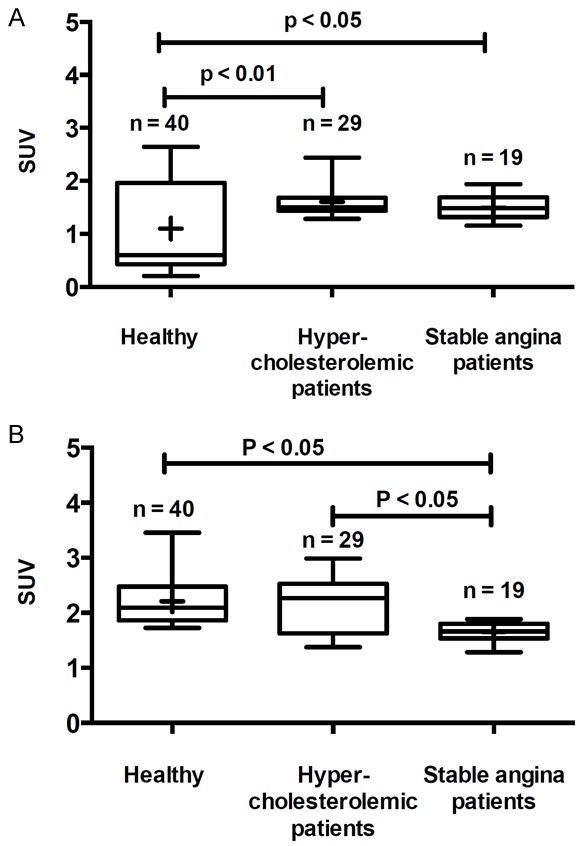
This study was aimed to investigate the usefulness of (18)F-FDG-PET to differentiate vascular inflammation and to determine the effect of rosuvastatin. Eight subjects were recruited and were divided according to their health status in three groups; 3 healthy subjects, 3 patients with hypercholesterolemia and 2 patients with stable angina pectoris. Hypercholesterolemic patients were submitted immediately after their recruitment to rosuvastatin treatment (20 mg/d). Two PET/CT measurements were made throughout the course of the study, one at baseline and the second 12 months later. Our results showed that the ratio of calcified arteries to total analyzed arteries segments were 23%, 36% and 44% for healthy, hypercholesterolemic and stable angina patients respectively. Healthy subjects present, at baseline, a high level of vascular inflammation as measured by (18)F-FDG uptake in both calcified and non-calcified segments of the arteries. This vascular inflammation increases as a function of the cardiovascular risk factors. After the 12-month follow-up period, non-calcified arteries showed a significant increase of (18)F-FDG uptake in both healthy, hypercholesterolemic and stable angina patients. However, the highest increase was noted for the healthy subjects; (50% increase, p<0.0001), while hypercholesterolemic patients under rosuvastatin showed only 25% increase of (18)F-FDG uptake (p<0.0001). This study confirms the usefulness of (18)F-FDG measurement to localize and quantify arterial inflammation in each artery segments and as a function of the CVD risk factors. Rosuvastatin may have a protective effect against arterial inflammation however; other studies with higher rosuvastatin doses (>20 mg/d) are needed to confirm this beneficial effect.
Keywords: 18F-FDG; Atherosclerosis; aging; positron emission tomography; rosuvastatin; vascular inflammation.
Figures
Similar articles
-
High Tyrosol and Hydroxytyrosol Intake Reduces Arterial Inflammation and Atherosclerotic Lesion Microcalcification in Healthy Older Populations.Antioxidants (Basel). 2024 Jan 22;13(1):130. doi: 10.3390/antiox13010130. Antioxidants (Basel). 2024. PMID: 38275655 Free PMC article.
-
Assessment of inflammation in large arteries with 18F-FDG-PET in elderly.Comput Med Imaging Graph. 2013 Oct-Dec;37(7-8):459-65. doi: 10.1016/j.compmedimag.2013.09.006. Epub 2013 Oct 5. Comput Med Imaging Graph. 2013. PMID: 24148785
-
Natural history of atherosclerotic disease progression as assessed by (18)F-FDG PET/CT.Int J Cardiovasc Imaging. 2016 Jan;32(1):49-59. doi: 10.1007/s10554-015-0660-8. Epub 2015 Apr 22. Int J Cardiovasc Imaging. 2016. PMID: 25898891
-
Thresholds for Arterial Wall Inflammation Quantified by 18F-FDG PET Imaging: Implications for Vascular Interventional Studies.JACC Cardiovasc Imaging. 2016 Oct;9(10):1198-1207. doi: 10.1016/j.jcmg.2016.04.007. Epub 2016 Sep 14. JACC Cardiovasc Imaging. 2016. PMID: 27639759 Free PMC article.
-
Variability and uncertainty of 18F-FDG PET imaging protocols for assessing inflammation in atherosclerosis: suggestions for improvement.J Nucl Med. 2015 Apr;56(4):552-9. doi: 10.2967/jnumed.114.142596. Epub 2015 Feb 26. J Nucl Med. 2015. PMID: 25722452 Review.
Cited by
-
Imaging Subclinical Atherosclerosis: Where Do We Stand?Curr Cardiol Rev. 2017;13(1):47-55. doi: 10.2174/1573403x12666160803095855. Curr Cardiol Rev. 2017. PMID: 27492229 Free PMC article. Review.
-
Inflammation, Atherosclerosis, and Coronary Artery Disease: PET/CT for the Evaluation of Atherosclerosis and Inflammation.Clin Med Insights Cardiol. 2015 Jan 7;8(Suppl 3):13-21. doi: 10.4137/CMC.S17063. eCollection 2014. Clin Med Insights Cardiol. 2015. PMID: 25674025 Free PMC article. Review.
-
Identifying Vulnerable Atherosclerotic Plaque in Rabbits Using DMSA-USPIO Enhanced Magnetic Resonance Imaging to Investigate the Effect of Atorvastatin.PLoS One. 2015 May 14;10(5):e0125677. doi: 10.1371/journal.pone.0125677. eCollection 2015. PLoS One. 2015. PMID: 25973795 Free PMC article.
-
High Tyrosol and Hydroxytyrosol Intake Reduces Arterial Inflammation and Atherosclerotic Lesion Microcalcification in Healthy Older Populations.Antioxidants (Basel). 2024 Jan 22;13(1):130. doi: 10.3390/antiox13010130. Antioxidants (Basel). 2024. PMID: 38275655 Free PMC article.
References
-
- Stern S, Behar S, Gottlieb S. Cardiology patient pages. Aging and diseases of the heart. Circulation. 2003;108:99–101. - PubMed
-
- Virmani R, Kolodgie FD, Burke AP, Finn AV, Gold HK, Tulenko TN, Wrenn SP, Narula J. Atherosclerotic plaque progression and vulnerability to rupture: angiogenesis as a source of intraplaque hemorrhage. Arterioscler Thromb Vasc Biol. 2005;25:2054–2061. - PubMed
-
- Jaffer FA, O’Donnell CJ, Larson MG, Chan SK, Kissinger KV, Kupka MJ, Salton C, Botnar RM, Levy D, Manning WJ. Age and sex distribution of subclinical aortic atherosclerosis: a magnetic resonance imaging examination of the Framingham Heart Study. Arterioscler Thromb Vasc Biol. 2002;22:849–854. - PubMed
-
- Smith SC Jr, Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, Grundy SM, Hiratzka L, Jones D, Krumholz HM, Mosca L, Pasternak RC, Pearson T, Pfeffer MA, Taubert KA. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the National Heart, Lung, and Blood Institute. Circulation. 2006;113:2363–2372. - PubMed
-
- Shah PK. Inflammation and plaque vulnerability. Cardiovasc Drugs Ther. 2009;23:31–40. - PubMed
LinkOut - more resources
Full Text Sources