

Psychological therapies for the management of chronic and recurrent pain in children and adolescents
- PMID: 24796681
- PMCID: PMC5886855
- DOI: 10.1002/14651858.CD003968.pub4
Psychological therapies for the management of chronic and recurrent pain in children and adolescents
Update in
-
Psychological therapies for the management of chronic and recurrent pain in children and adolescents.Cochrane Database Syst Rev. 2018 Sep 29;9(9):CD003968. doi: 10.1002/14651858.CD003968.pub5. Cochrane Database Syst Rev. 2018. PMID: 30270423 Free PMC article.
Abstract
Background: This is an update of the original Cochrane review first published in Issue 1, 2003, and previously updated in 2009 and 2012. Chronic pain affects many children, who report severe pain, disability, and distressed mood. Psychological therapies are emerging as effective interventions to treat children with chronic or recurrent pain. This update focuses specifically on psychological therapies delivered face-to-face, adds new randomised controlled trials (RCTs), and additional data from previously included trials.
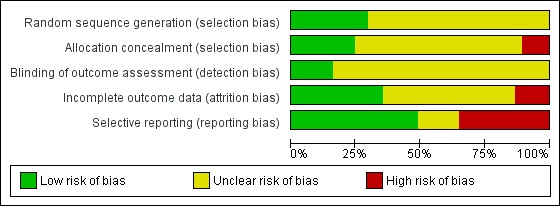
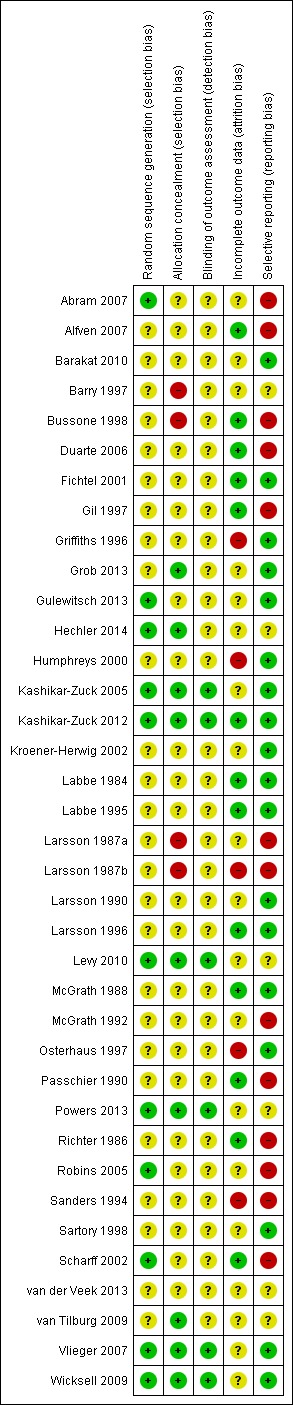
Objectives: There were three objectives to this review. First, to determine the effectiveness on clinical outcomes of pain severity, disability, depression, and anxiety of psychological therapy delivered face-to-face for chronic and recurrent pain in children and adolescents compared with active treatment, waiting-list, or standard medical care. Second, to evaluate the impact of psychological therapies on depression and anxiety, which were previously combined as 'mood'. Third, we assessed the risk of bias of the included studies and the quality of outcomes using the GRADE criteria.
Search methods: Searches were undertaken of CENTRAL, MEDLINE, EMBASE, and PsycINFO. We searched for further RCTs in the references of all identified studies, meta-analyses, and reviews. Trial registry databases were also searched. The date of most recent search was January 2014.
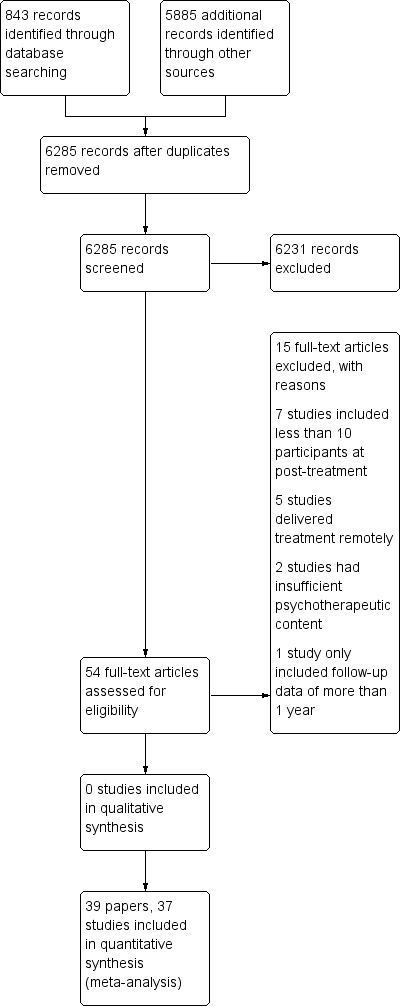
Selection criteria: RCTs with at least 10 participants in each arm post-treatment comparing psychological therapies with active treatment, standard medical care, or waiting-list control for children or adolescents with episodic, recurrent or persistent pain were eligible for inclusion. Only trials conducted in person (face-to-face) were considered. Studies that delivered treatment remotely were excluded from this update.
Data collection and analysis: All included studies were analysed and the quality of outcomes were assessed. All treatments were combined into one class, psychological treatments. Pain conditions were split into headache and non-headache. Both conditions were assessed on four outcomes: pain, disability, depression, and anxiety. Data were extracted at two time points; post-treatment (immediately or the earliest data available following end of treatment) and at follow-up (between three and 12 months post-treatment).
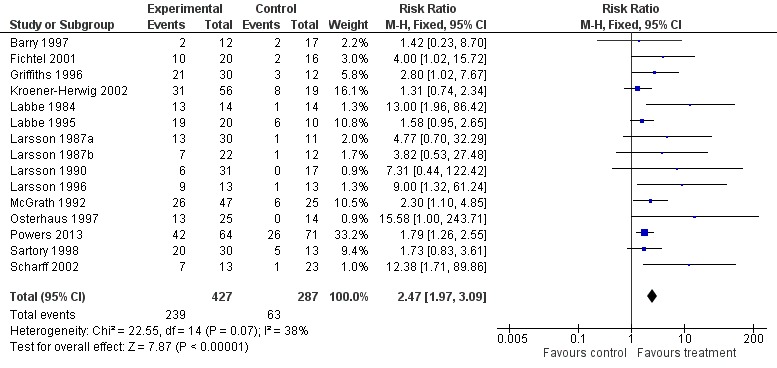
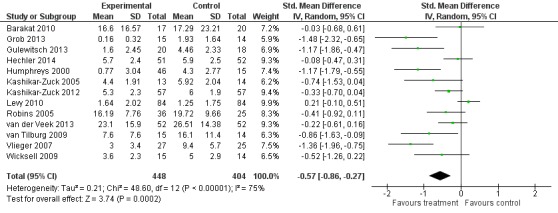
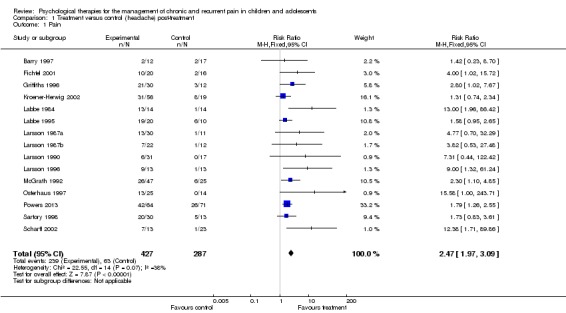
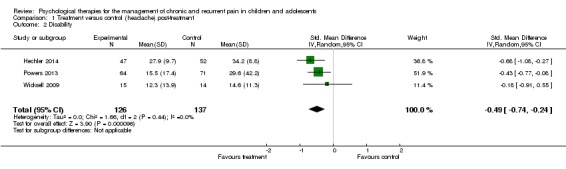
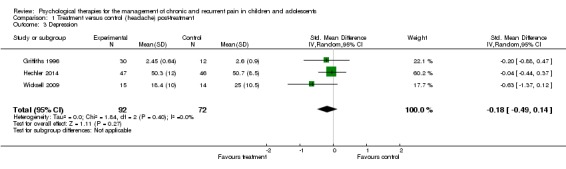
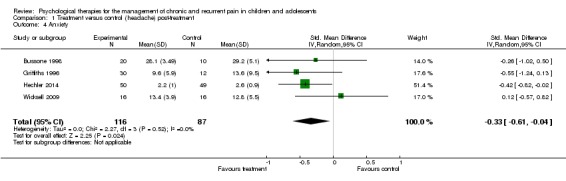
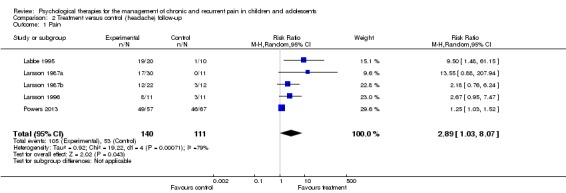
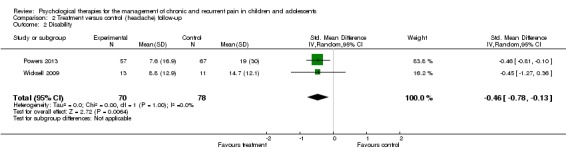
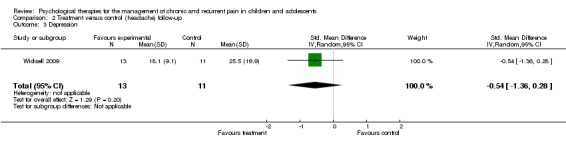
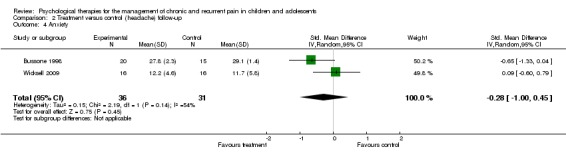
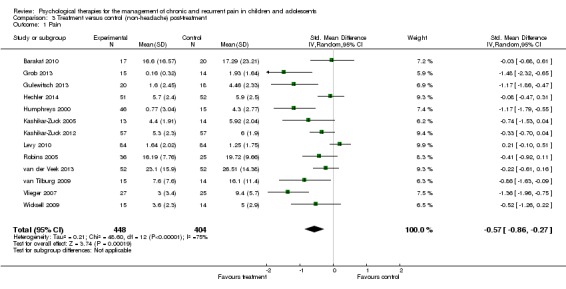
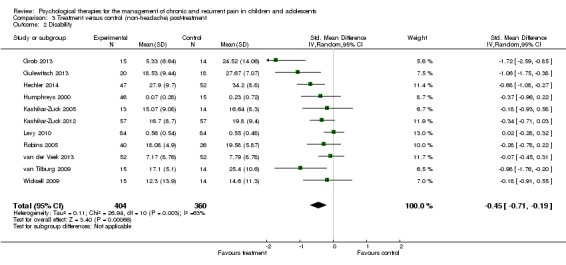
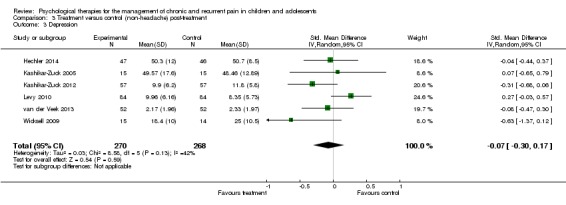
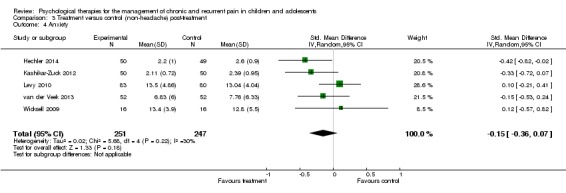
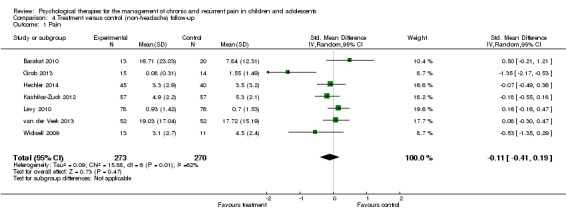
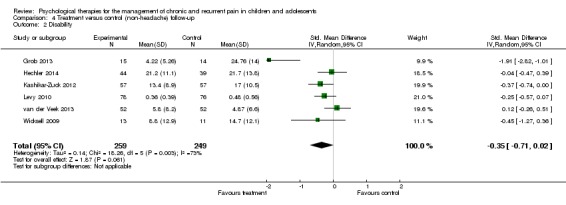
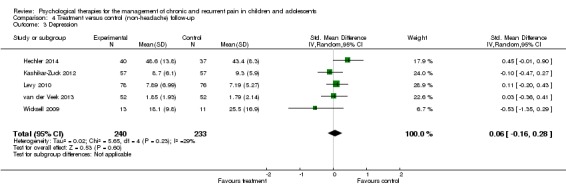
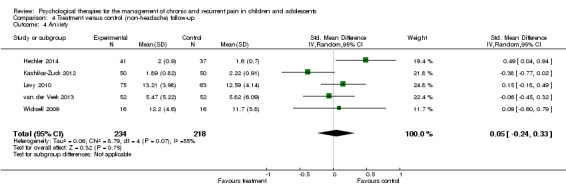
Main results: Seven papers were identified in the updated search. Of these papers, five presented new trials and two presented follow-up data for previously included trials. Five studies that were previously included in this review were excluded as therapy was delivered remotely. The review thus included a total of 37 studies. The total number of participants completing treatments was 2111. Twenty studies addressed treatments for headache (including migraine); nine for abdominal pain; two for mixed pain conditions including headache pain, two for fibromyalgia, two for recurrent abdominal pain or irritable bowel syndrome, and two for pain associated with sickle cell disease.Analyses revealed psychological therapies to be beneficial for children with chronic pain on seven outcomes. For headache pain, psychological therapies reduced pain post-treatment and at follow-up respectively (risk ratio (RR) 2.47, 95% confidence interval (CI) 1.97 to 3.09, z = 7.87, p < 0.01, number needed to treat to benefit (NNTB) = 2.94; RR 2.89, 95% CI 1.03 to 8.07, z = 2.02, p < 0.05, NNTB = 3.67). Psychological therapies also had a small beneficial effect at reducing disability in headache conditions post-treatment and at follow-up respectively (standardised mean difference (SMD) -0.49, 95% CI -0.74 to -0.24, z = 3.90, p < 0.01; SMD -0.46, 95% CI -0.78 to -0.13, z = 2.72, p < 0.01). No beneficial effect was found on depression post-treatment (SMD -0.18, 95% CI -0.49 to 0.14, z = 1.11, p > 0.05). At follow-up, only one study was eligible, therefore no analysis was possible and no conclusions can be drawn. Analyses revealed a small beneficial effect for anxiety post-treatment (SMD -0.33, 95% CI -0.61 to -0.04, z = 2.25, p < 0.05). However, this was not maintained at follow-up (SMD -0.28, 95% CI -1.00 to 0.45; z = 0.75, p > 0.05).Analyses revealed two beneficial effects of psychological treatment for children with non-headache pain. Pain was found to improve post-treatment (SMD -0.57, 95% CI -0.86 to -0.27, z = 3.74, p < 0.01), but not at follow-up (SMD -0.11, 95% CI -0.41 to 0.19, z = 0.73, p > 0.05). Psychological therapies also had a beneficial effect for disability post-treatment (SMD -0.45, 95% CI -0.71 to -0.19, z = 3.40, p < 0.01), but this was not maintained at follow-up (SMD -0.35, 95% CI -0.71 to 0.02, z = 1.87, p > 0.05). No effect was found for depression or anxiety post-treatment (SMD -0.07, 95% CI -0.30 to 0.17, z = 0.54, p > 0.05; SMD -0.15, 95% CI -0.36 to 0.07, z = 1.33, p > 0.05) or at follow-up (SMD 0.06, 95% CI -0.16 to 0.28, z = 0.53, p > 0.05; SMD 0.05, 95% CI -0.24 to 0.33, z = 0.32, p > 0.05).
Authors' conclusions: Psychological treatments delivered face-to-face are effective in reducing pain intensity and disability for children and adolescents (<18 years) with headache, and therapeutic gains appear to be maintained, although this should be treated with caution for the disability outcome as only two studies could be included in the follow-up analysis. Psychological therapies are also beneficial at reducing anxiety post-treatment for headache. For non-headache conditions, psychological treatments were found to be beneficial for pain and disability post-treatment but these effects were not maintained at follow-up. There is limited evidence available to estimate the effects of psychological therapies on depression and anxiety for children and adolescents with headache and non-headache pain. The conclusions of this update replicate and add to those of the previous review which found that psychological therapies were effective in reducing pain intensity for children with headache and non-headache pain conditions, and these effects were maintained at follow-up for children with headache conditions.
Conflict of interest statement
None known.
Figures
Update of
-
Psychological therapies for the management of chronic and recurrent pain in children and adolescents.Cochrane Database Syst Rev. 2012 Dec 12;12:CD003968. doi: 10.1002/14651858.CD003968.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 May 05;(5):CD003968. doi: 10.1002/14651858.CD003968.pub4. PMID: 23235601 Free PMC article. Updated.
References
References to studies included in this review
-
- Abram HS, Buckloh LM, Schilling LS, Armatti Wiltrout S, Ramirez‐Garnica G, Turk WR. A randomized, controlled trail of a neurological and psychoeducational group appointment model for pediatric headaches. Children's Healthcare 2007;36:249‐65.
-
- Alfven G, Lindstrom A. A new method for the treatment of recurrent abdominal pain of prolonged negative stress origin. Acta Paediatrica 2007;96:76‐81. - PubMed
-
- Barry J, Baeyer CL. Brief cognitive‐behavioral group treatment for children's headache. Clinical Journal of Pain 1997;13:215‐20. - PubMed
-
- Bussone G, Grazzi L, D'Amico D, Leone M, Andrasik F. Biofeedback‐assisted relaxation training for young adolescents with tension‐type headache: a controlled study. Cephalalgia 1988;18:463‐7. - PubMed
References to studies excluded from this review
-
- Connelly M, Rapoff MA, Thompson N, Connelly W. Headstrong: a pilot study of a CD‐ROM intervention for recurrent pediatric headache. Journal of Pediatric Psychology 2006;31:737‐47. - PubMed
-
- Fentress DW, Masek BJ, Mehegan JE, Benson H. Biofeedback and relaxation‐response training in the treatment of pediatric migraine. Developmental Medicine and Child Neurology 1986;28:139‐46. - PubMed
-
- Hicks CL, Baeyer CL, McGrath PJ. Online psychological treatment for pediatric recurrent pain: a randomized evaluation. Journal of Pediatric Psychology 2006;31:724‐36. - PubMed
-
- Koenig J, Oelkers‐Ax R, Kaess M, Parzer P, Lenzen C, Hillecke TK, et al. Specific music therapy techniques in the treatment of primary headache disorders in adolescents: a randomized attention‐placebo‐controlled trial. Journal of Pain 2013;14(10):1196‐207. - PubMed
-
- Kroner‐Herwig B, Mohn U, Pothmann R. Comparison of biofeedback and relaxation in the treatment of pediatric headache and the influence of parent involvement on outcome. Applied Psychophysiology and Biofeedback 1998;23:143‐57. - PubMed
Additional references
-
- Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, Vist GE, Falck‐Ytter Y, Meerpohl J, Norris S, Guyatt GH. GRADE guidelines: 3. Rating the quality of evidence. Journal of Clinical Epidemiolgy 2011;64:401‐6. - PubMed
-
- Bursch B, Walco GA, Zeltzer L. Clinical assessment and management of chronic pain and pain‐associated disability syndrome. Developmental and Behavioral Pediatrics 1998;19:45‐53. - PubMed
-
- Cohen J. A power primer. Psychological Bulletin 1992;112(1):155‐9. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical