

Anti-HMGCR autoantibodies in European patients with autoimmune necrotizing myopathies: inconstant exposure to statin
- PMID: 24797170
- PMCID: PMC4632910
- DOI: 10.1097/MD.0000000000000028
Anti-HMGCR autoantibodies in European patients with autoimmune necrotizing myopathies: inconstant exposure to statin
Abstract
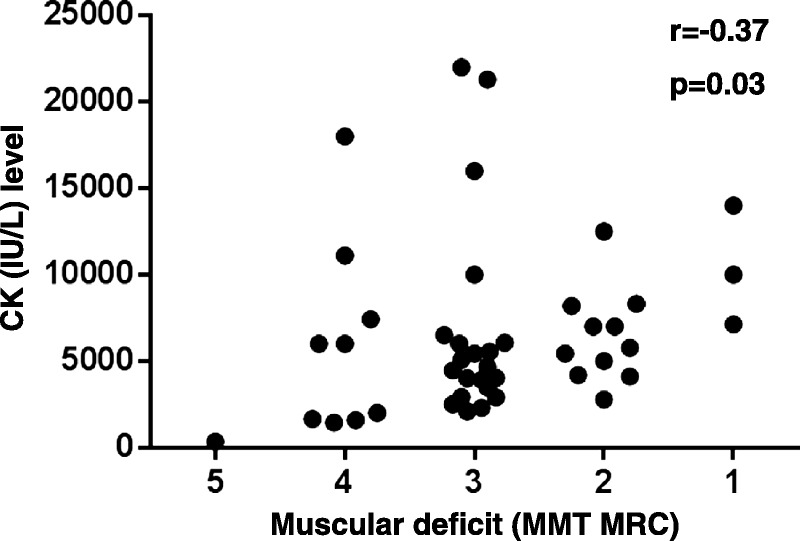
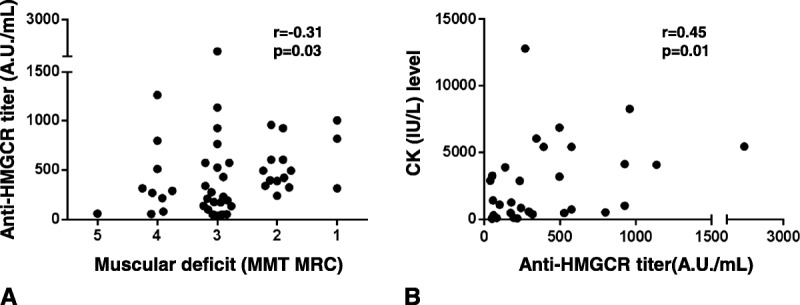
Necrotizing autoimmune myopathy (NAM) is a group of acquired myopathies characterized by prominent myofiber necrosis with little or no muscle inflammation. Recently, researchers identified autoantibodies (aAb) against 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR) in patients with NAM, especially in statin-exposed patients. Here we report what is to our knowledge the first European cohort of patients with NAM.The serum of 206 patients with suspicion of NAM was tested for detection of anti-HMGCR aAb using an addressable laser bead immunoassay. Forty-five patients were found to be anti-HMGCR positive. Their mean age was 48.9 ± 21.9 years and the group was predominantly female (73.3%). Statin exposure was recorded in 44.4% of patients. Almost all patients had a muscular deficit (97.7%), frequently severe (Medical Research Council [MRC] 5 ≤3 in 75.5%). Subacute onset (<6 mo) was noted for most of them (64.4%). Nevertheless, 3 patients (6.6%) had a slowly progressive course over more than 10 years. Except for weight loss (20%), no extramuscular sign was observed. The mean CK level was high (6941 ± 8802 IU/L) and correlated with muscle strength evaluated by manual muscle testing (r = -0.37, p = 0.03). Similarly, anti-HMGCR aAb titers were correlated with muscular strength (r = -0.31; p = 0.03) and CK level (r = 0.45; p = 0.01). Mean duration of treatment was 34.1 ± 40.8 months, and by the end of the study no patient had been able to stop treatment.This study confirms the observation and description of anti-HMGCR aAb associated with NAM. The majority of patients were statin naive and needed prolonged treatments. Some patients had a dystrophic-like presentation. Anti-HMGR aAb titers correlated with CK levels and muscle strength, suggesting their pathogenic role.
Figures
References
-
- Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, Healey LA, Kaplan SR, Liang MH, Luthra HS, Medsger TA, Jr, Mitchell DM, Neustadt DH, Pinals RS, Schaller JG, Sharp JT, Wilder RL, Hunder GG. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis.Arthritis Rheum. 1988;31:315–324. - PubMed
-
- Benveniste O, Drouot L, Jouen F, Charuel JL, Bloch-Queyrat C, Behin A, Amoura Z, Marie I, Guiguet M, Eymard B, Gilbert D, Tron F, Herson S, Musset L, Boyer O. Correlation of anti-signal recognition particle autoantibody levels with creatine kinase activity in patients with necrotizing myopathy. Arthritis Rheum. 2011;63: 1961– 1971. - PubMed
-
- Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975; 292: 344– 347. - PubMed
-
- Bronner IM, Hoogendijk JE, Wintzen AR, van der Meulen MF, 9Linssen WH, Wokke JH, de Visser M. Necrotising myopathy, an unusual presentation of a steroid-responsive myopathy. J Neurol. 2003; 250: 480– 485. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
