

Familial Mediterranean fever: genotype-phenotype correlations in Japanese patients
- PMID: 24797171
- PMCID: PMC4632911
- DOI: 10.1097/MD.0000000000000029
Familial Mediterranean fever: genotype-phenotype correlations in Japanese patients
Abstract
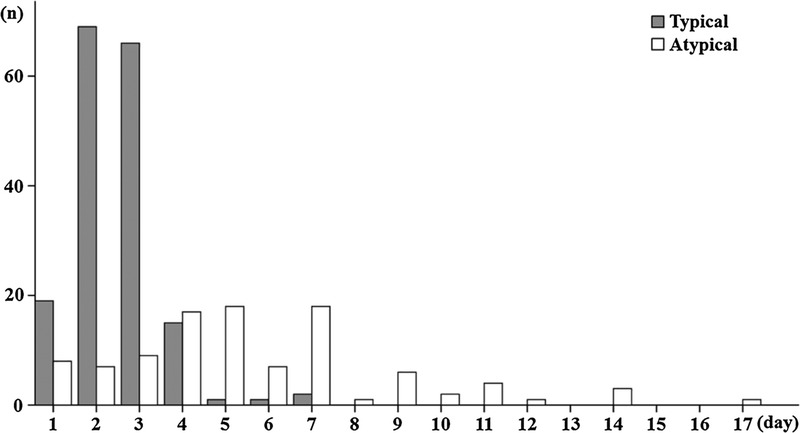
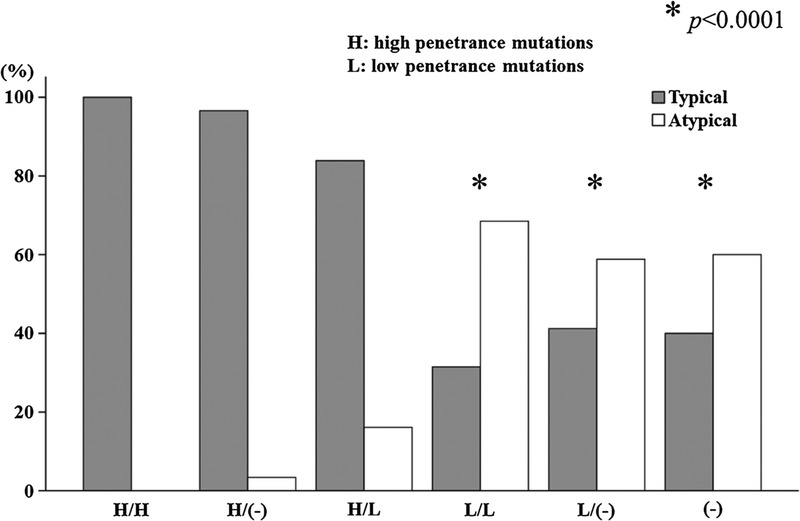
Familial Mediterranean fever (FMF) is an autoinflammatory disease caused by MEditerranean FeVer gene (MEFV) mutations. In Japan, patients with FMF have been previously reported, including a mild or incomplete form. Several factors are presumed to contribute to the variable penetrance and to the phenotypic variability of FMF. We conducted the current study to investigate the correlation of variable clinical presentations and MEFV genotypic distributions in Japanese FMF patients.We analyzed demographic, clinical, and genetic data for 311 FMF patients enrolled in the study. Clinically, we classified FMF into 2 phenotypes: 1) the "typical" form of FMF, and 2) the "atypical" form of FMF according to the Tel Hashomer criteria. Patients with the typical FMF phenotype had a higher frequency of febrile episodes, a shorter duration of febrile attacks, more frequent thoracic pain, abdominal pain, a family history of FMF, and MEFV exon 10 mutations. Conversely, patients with the atypical FMF phenotype had a lower frequency of fever episodes and more frequent arthritis in atypical distribution, myalgia, and MEFV exon 3 mutations. Multivariate analysis showed that the variable associated with typical FMF presentation was the presence of MEFV exon 10 mutations. Typical FMF phenotype frequencies were decreased in patients carrying 2 or a single low-penetrance mutations compared with those carrying 2 or a single high-penetrance mutations (M694I), with an opposite trend for the atypical FMF phenotype. In addition, patients having more than 2 MEFV mutations had a younger disease onset and a higher prevalence of thoracic pain than those carrying a single or no mutations. Thus, MEFV exon 10 mutations are associated with the more typical FMF phenotype. In contrast, more than half of the Japanese FMF patients without MEFV exon 10 mutations presented with an atypical FMF phenotype, indicating that Japanese FMF patients tend to be divided into 2 phenotypes by a variation of MEFV mutations.
Figures
References
-
- Ancient missense mutations in a new member of the RoRet gene family are likely to cause familial Mediterranean fever. The International FMF Consortium. Cell. 1997; 90: 797– 807. - PubMed
-
- Ben-Chetrit E, Levy M. Familial Mediterranean fever. Lancet. 1998; 351: 659– 664. - PubMed
-
- Ben-Chetrit E, Peleg H, Aamar S, Heyman SN. The spectrum of MEFV clinical presentations—is it familial Mediterranean fever only? Rheumatology (Oxford). 2009; 48: 1455– 1459. - PubMed
-
- Booth DR, Gillmore JD, Lachmann HJ, Booth SE, Bybee A, Soyturk M, Akar S, Pepys MB, Tunca M, Hawkins PN. The genetic basis of autosomal dominant familial Mediterranean fever. QJM. 2000; 93: 217– 221. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
