

Successful anti-scavenger receptor class B type I (SR-BI) monoclonal antibody therapy in humanized mice after challenge with HCV variants with in vitro resistance to SR-BI-targeting agents
- PMID: 24797654
- PMCID: PMC4211977
- DOI: 10.1002/hep.27196
Successful anti-scavenger receptor class B type I (SR-BI) monoclonal antibody therapy in humanized mice after challenge with HCV variants with in vitro resistance to SR-BI-targeting agents
Abstract
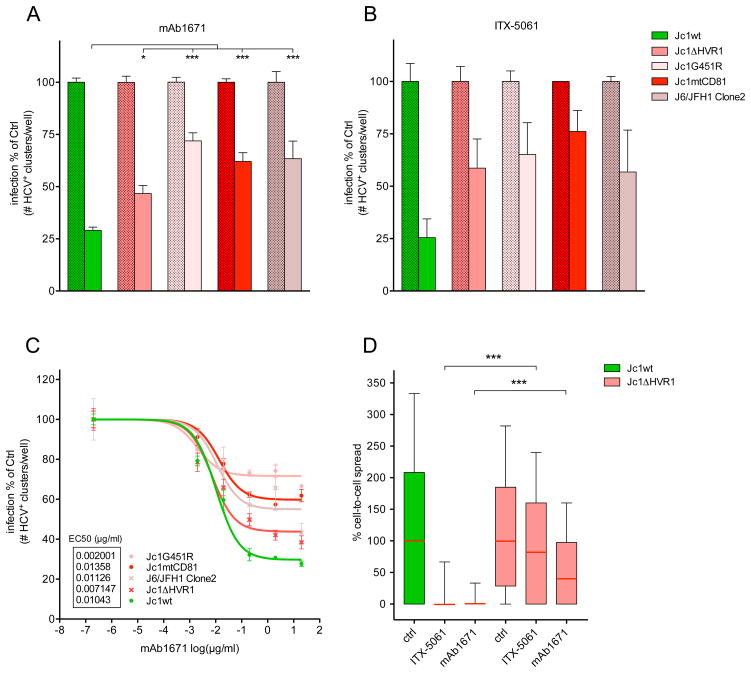
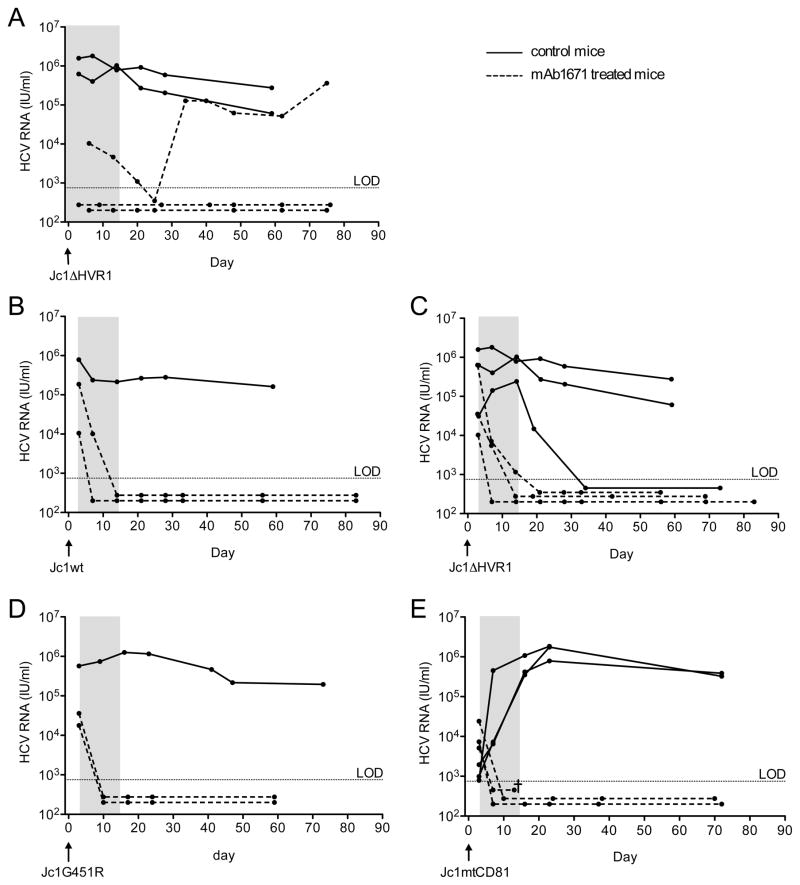
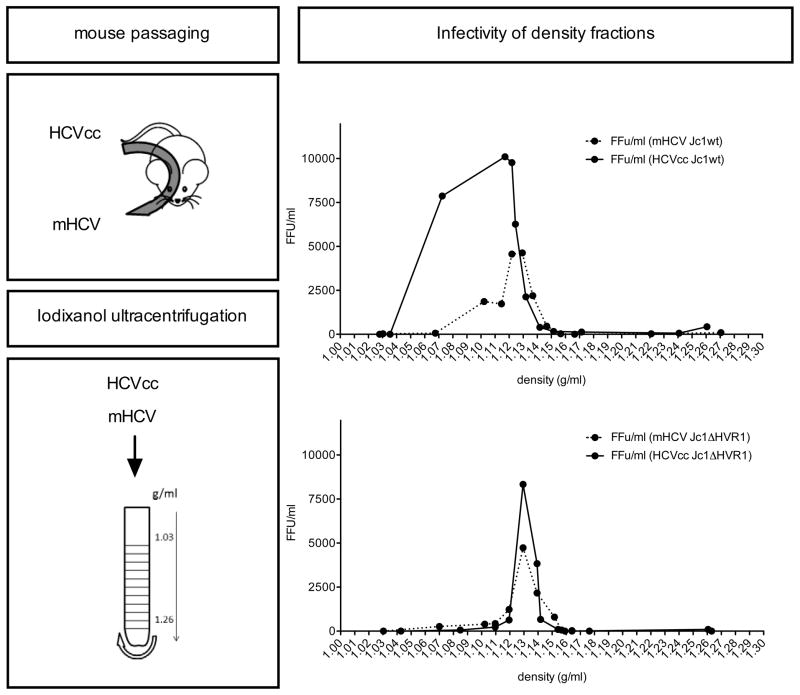
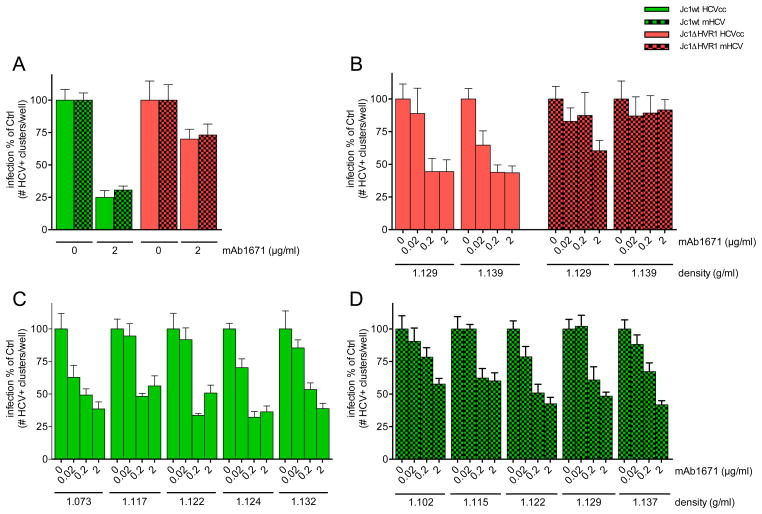
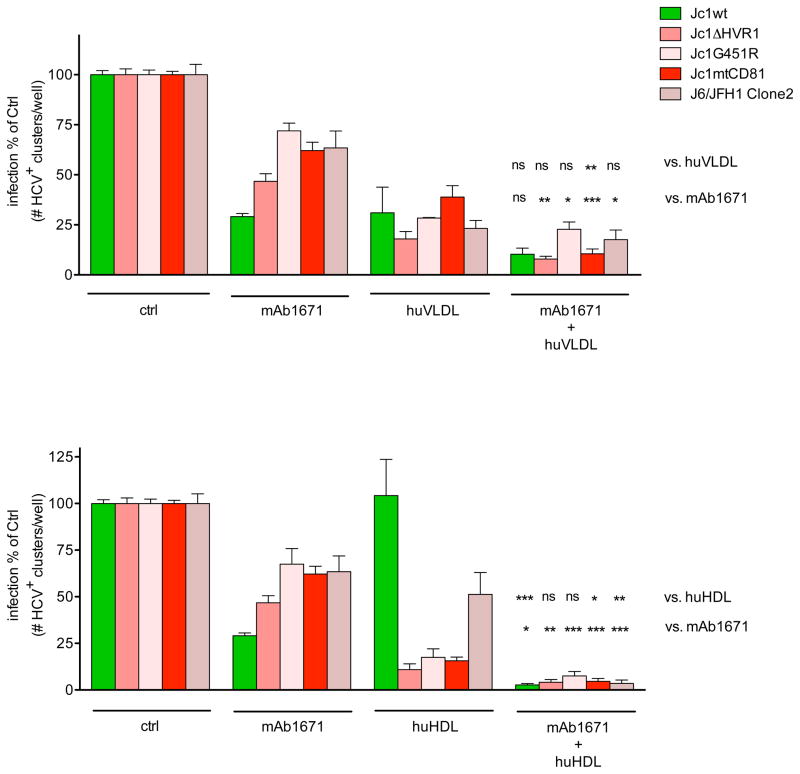
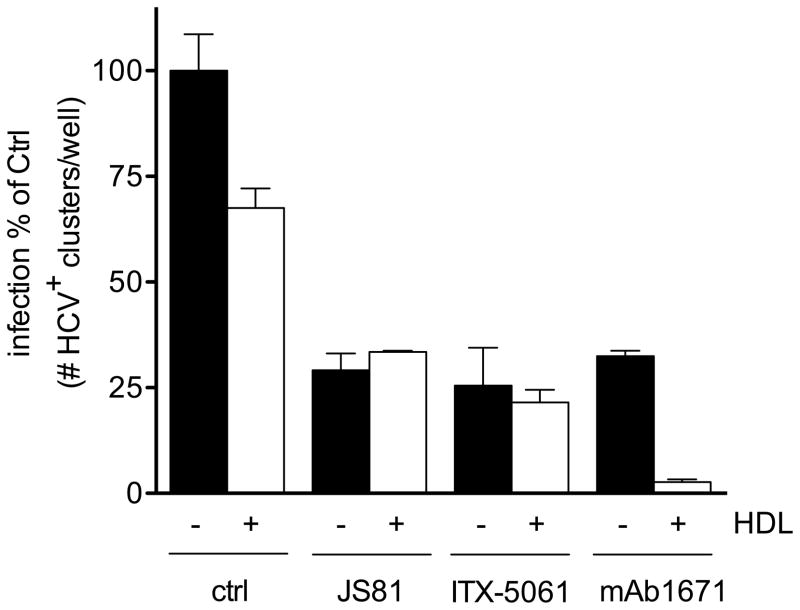
Hepatitis C virus (HCV)-induced endstage liver disease is currently a major indication for liver transplantation. After transplantation the donor liver inevitably becomes infected with the circulating virus. Monoclonal antibodies (mAbs) against the HCV coreceptor scavenger receptor class B type I (SR-BI) inhibit HCV infection of different genotypes, both in cell culture and in humanized mice. Anti-SR-BI mAb therapy is successful even when initiated several days after HCV exposure, supporting its potential applicability to prevent HCV reinfection of liver allografts. However, HCV variants with reduced SR-BI dependency have been described in the literature, which could potentially limit the use of SR-BI targeting therapy. In this study we show, both in a preventative and postexposure setting, that humanized mice infected with HCV variants exhibiting increased in vitro resistance to SR-BI-targeting molecules remain responsive to anti-SR-BI mAb therapy in vivo. A 2-week antibody therapy readily cleared HCV RNA from the circulation of infected humanized mice. We found no evidence supporting increased SR-BI-receptor dependency of viral particles isolated from humanized mice compared to cell culture-produced virus. However, we observed that, unlike wild-type virus, the in vitro infectivity of the resistant variants was inhibited by both human high density lipoprotein (HDL) and very low density lipoprotein (VLDL). The combination of mAb1671 with these lipoproteins further increased the antiviral effect.
Conclusion: HCV variants that are less dependent on SR-BI in vitro can still be efficiently blocked by an anti-SR-BI mAb in humanized mice. Since these variants are also more susceptible to neutralization by anti-HCV envelope antibodies, their chance of emerging during anti-SR-BI therapy is severely reduced. Our data indicate that anti-SR-BI receptor therapy could be an effective way to prevent HCV infection in a liver transplant setting.
© 2014 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Nothing to disclose.
Figures
Comment in
-
Antibodies to the high-density lipoprotein receptor SR-B1 potently inhibit hepatitis C virus replication in vivo: New avenues for preventing reinfection of the liver following transplantation.Hepatology. 2014 Nov;60(5):1463-5. doi: 10.1002/hep.27276. Epub 2014 Sep 18. Hepatology. 2014. PMID: 24962233 Free PMC article. No abstract available.
References
-
- Zeuzem S. Interferon-based therapy for chronic hepatitis C: current and future perspectives. Nat Clin Pract Gastroenterol Hepatol. 2008;5:610–622. - PubMed
-
- Sarrazin C, Hezode C, Zeuzem S, Pawlotsky JM. Antiviral strategies in hepatitis C virus infection. J Hepatol. 2012;56 (Suppl 1):S88–100. - PubMed
-
- Peveling-Oberhag J, Zeuzem S, Hofmann WP. Antiviral therapy of chronic hepatitis C in patients with advanced liver disease and after liver transplantation. Med Microbiol Immunol. 2010;199:1–10. - PubMed
-
- Charlton M. Telaprevir, boceprevir, cytochrome P450 and immunosuppressive agents - A potentially lethal cocktail. Hepatology. 2011;54:3–5. - PubMed
-
- Rubin A, Aguilera V, Berenguer M. Liver transplantation and hepatitis C. Clin Res Hepatol Gastroenterol. 2011;35:805–812. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials