

Individualization of piperacillin dosing for critically ill patients: dosing software to optimize antimicrobial therapy
- PMID: 24798288
- PMCID: PMC4068511
- DOI: 10.1128/AAC.02664-14
Individualization of piperacillin dosing for critically ill patients: dosing software to optimize antimicrobial therapy
Abstract
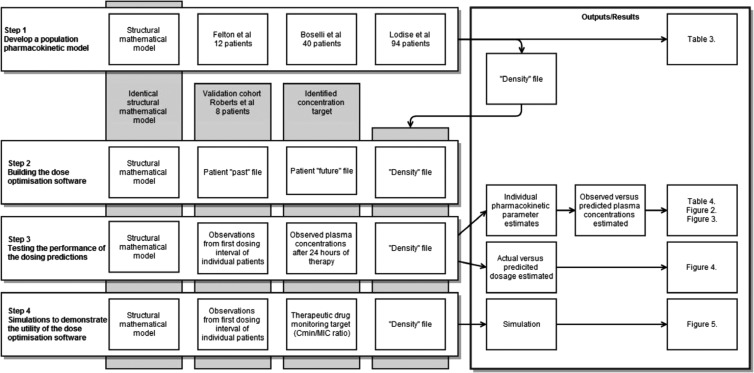
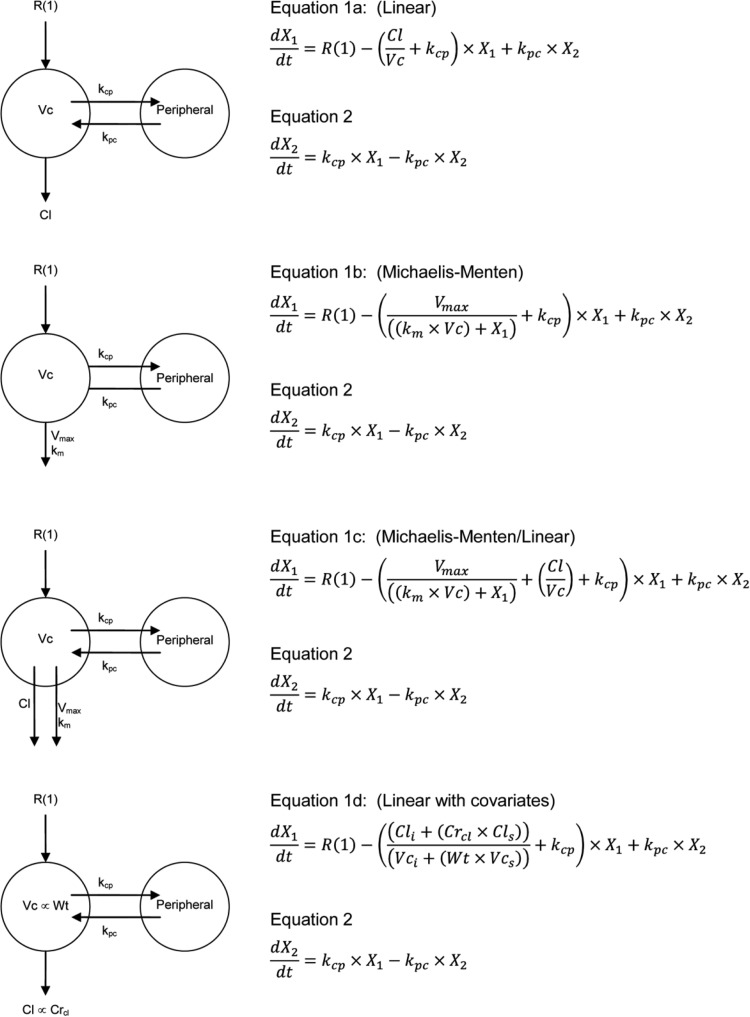
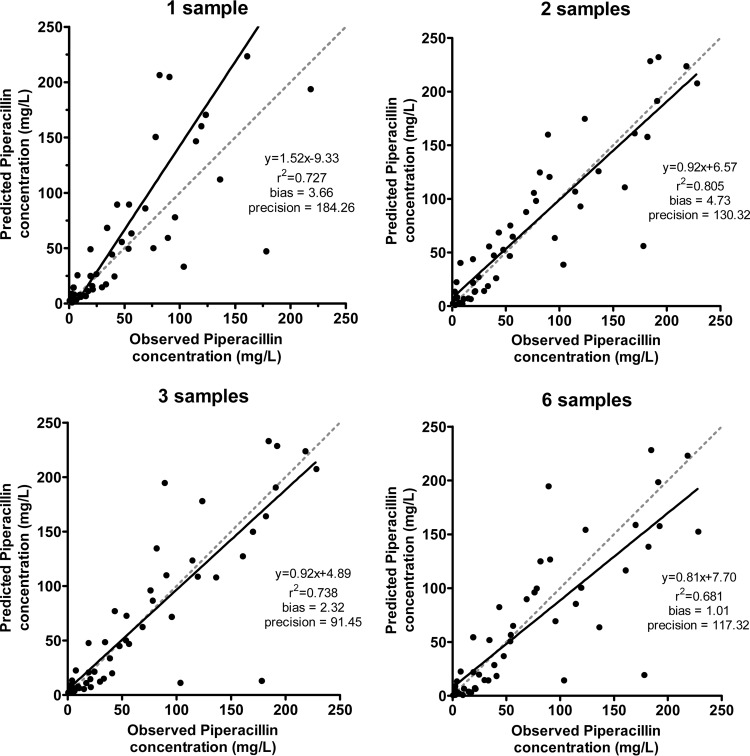
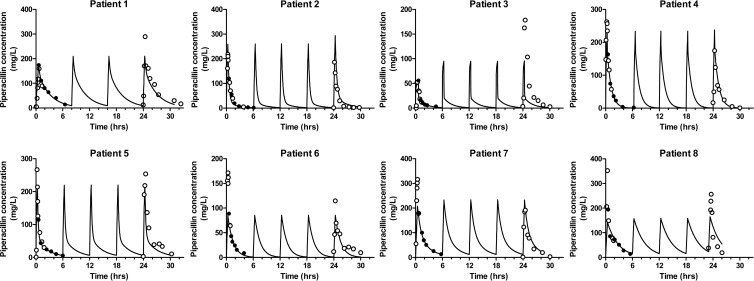
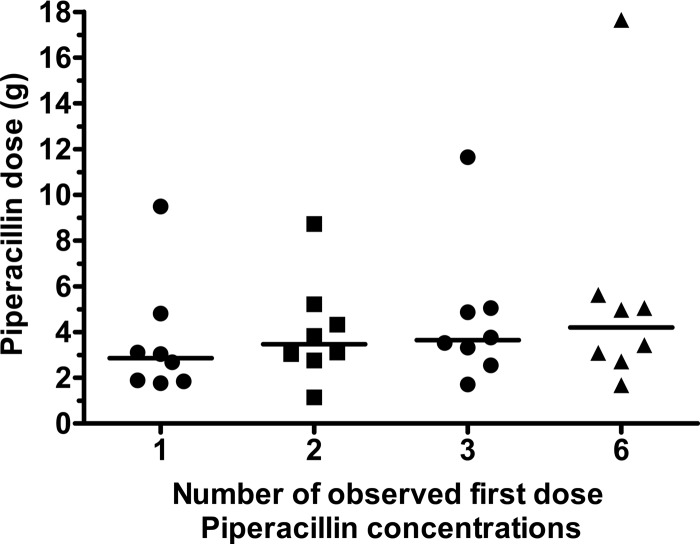
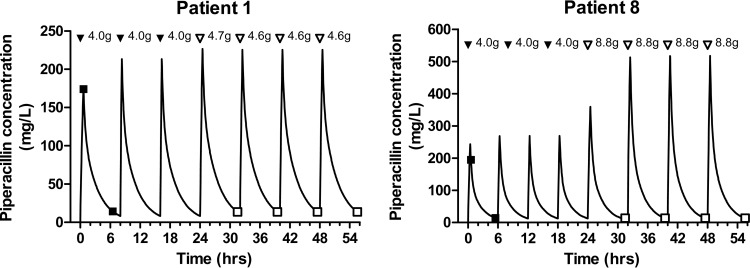
Piperacillin-tazobactam is frequently used for empirical and targeted therapy of infections in critically ill patients. Considerable pharmacokinetic (PK) variability is observed in critically ill patients. By estimating an individual's PK, dosage optimization Bayesian estimation techniques can be used to calculate the appropriate piperacillin regimen to achieve desired drug exposure targets. The aim of this study was to establish a population PK model for piperacillin in critically ill patients and then analyze the performance of the model in the dose optimization software program BestDose. Linear, with estimated creatinine clearance and weight as covariates, Michaelis-Menten (MM) and parallel linear/MM structural models were fitted to the data from 146 critically ill patients with nosocomial infection. Piperacillin concentrations measured in the first dosing interval, from each of 8 additional individuals, combined with the population model were embedded into the dose optimization software. The impact of the number of observations was assessed. Precision was assessed by (i) the predicted piperacillin dosage and by (ii) linear regression of the observed-versus-predicted piperacillin concentrations from the second 24 h of treatment. We found that a linear clearance model with creatinine clearance and weight as covariates for drug clearance and volume of distribution, respectively, best described the observed data. When there were at least two observed piperacillin concentrations, the dose optimization software predicted a mean piperacillin dosage of 4.02 g in the 8 patients administered piperacillin doses of 4.00 g. Linear regression of the observed-versus-predicted piperacillin concentrations for 8 individuals after 24 h of piperacillin dosing demonstrated an r(2) of >0.89. In conclusion, for most critically ill patients, individualized piperacillin regimens delivering a target serum piperacillin concentration is achievable. Further validation of the dosage optimization software in a clinical trial is required.
Copyright © 2014 Felton et al.
Figures
References
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M. 2006. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 34:1589–1596. 10.1097/01.CCM.0000217961.75225.E9 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
