

Economic return from the Women's Health Initiative estrogen plus progestin clinical trial: a modeling study
- PMID: 24798522
- PMCID: PMC4157355
- DOI: 10.7326/M13-2348
Economic return from the Women's Health Initiative estrogen plus progestin clinical trial: a modeling study
Abstract
Background: The findings of the Women's Health Initiative (WHI) estrogen plus progestin (E+P) trial led to a substantial reduction in use of combined hormone therapy (cHT) among postmenopausal women in the United States. The economic effect of this shift has not been evaluated relative to the trial's $260 million cost (2012 U.S. dollars).
Objective: To estimate the economic return from the WHI E+P trial.
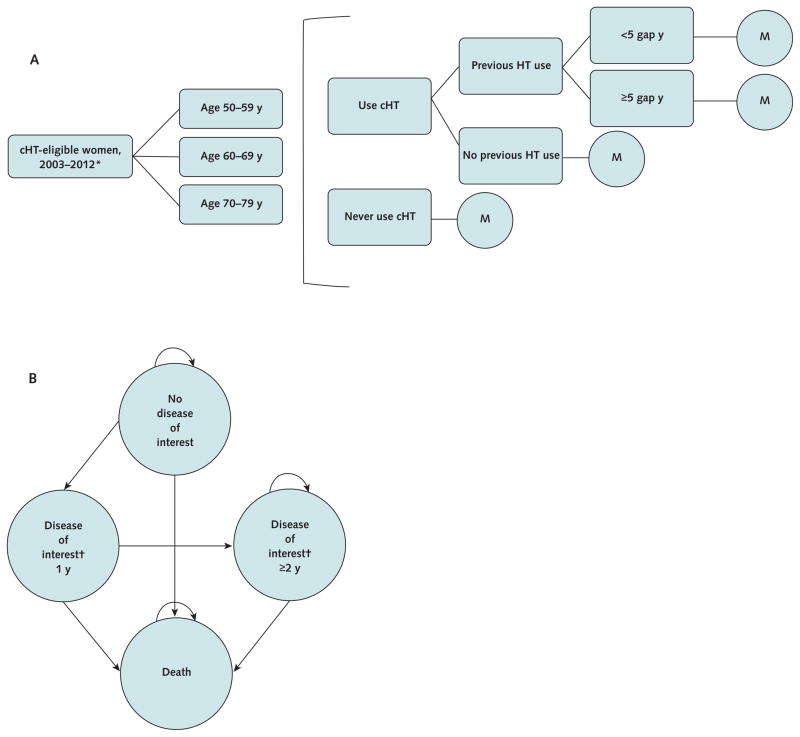
Design: Decision model to simulate health outcomes for a "WHI scenario" with observed cHT use and a "no-WHI scenario" with cHT use extrapolated from the pretrial period.
Data sources: Primary analyses of WHI outcomes, peer-reviewed literature, and government sources.
Target population: Postmenopausal women in the United States, aged 50 to 79 years, who did not have a hysterectomy.
Time horizon: 2003 to 2012.
Perspective: Payer.
Intervention: Combined hormone therapy.
Outcome measures: Disease incidence, expenditure, quality-adjusted life-years, and net economic return.
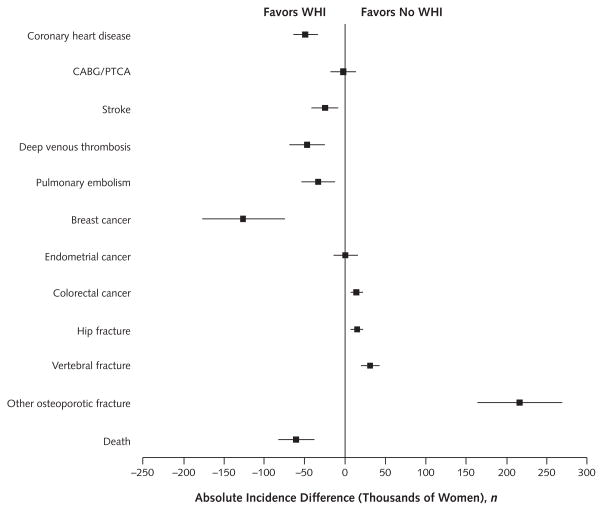
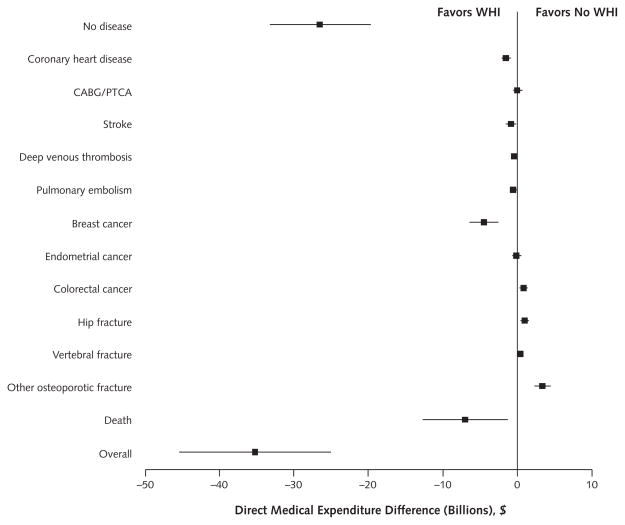
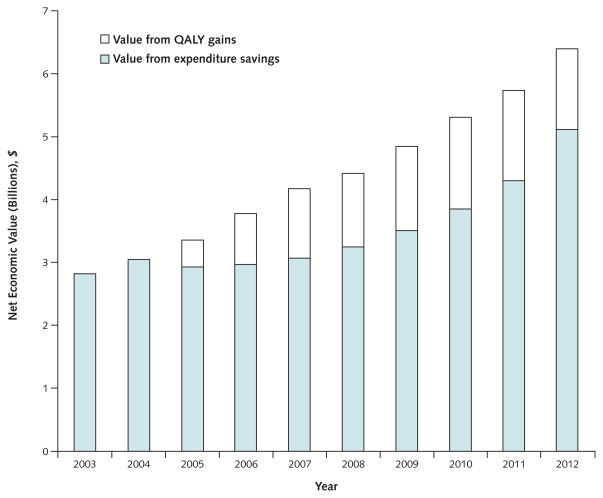
Results of base-case analysis: The WHI scenario resulted in 4.3 million fewer cHT users, 126,000 fewer breast cancer cases, 76,000 fewer cardiovascular disease cases, 263,000 more fractures, 145,000 more quality-adjusted life-years, and expenditure savings of $35.2 billion. The corresponding net economic return of the trial was $37.1 billion ($140 per dollar invested in the trial) at a willingness-to-pay level of $100,000 per quality-adjusted life-year.
Results of sensitivity analysis: The 95% CI for the net economic return of the trial was $23.1 to $51.2 billion.
Limitation: No evaluation of indirect costs or outcomes beyond 2012.
Conclusion: The WHI E+P trial made high-value use of public funds with a substantial return on investment. These results can contribute to discussions about the role of public funding for large, prospective trials with high potential for public health effects.
Primary funding source: National Heart, Lung, and Blood Institute.
Figures
Comment in
-
Investing in clinical science: make way for (not-so-uncommon) outliers.Ann Intern Med. 2014 May 6;160(9):651-2. doi: 10.7326/M14-0655. Ann Intern Med. 2014. PMID: 24798528 No abstract available.
References
-
- Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288:321–33. - PubMed
-
- Steinkellner AR, Denison SE, Eldridge SL, Lenzi LL, Chen W, Bowlin SJ. A decade of postmenopausal hormone therapy prescribing in the United States: long-term effects of the Women’s Health Initiative. Menopause. 2012;19:616–21. - PubMed
-
- Burkman RT, Collins JA, Greene RA. Current perspectives on benefits and risks of hormone replacement therapy. Am J Obstet Gynecol. 2001;185:S13–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials