

Active idiotypic vaccination versus control immunotherapy for follicular lymphoma
- PMID: 24799467
- PMCID: PMC4039868
- DOI: 10.1200/JCO.2012.43.9273
Active idiotypic vaccination versus control immunotherapy for follicular lymphoma
Abstract
Purpose: Idiotypes (Ids), the unique portions of tumor immunoglobulins, can serve as targets for passive and active immunotherapies for lymphoma. We performed a multicenter, randomized trial comparing a specific vaccine (MyVax), comprising Id chemically coupled to keyhole limpet hemocyanin (KLH) plus granulocyte macrophage colony-stimulating factor (GM-CSF) to a control immunotherapy with KLH plus GM-CSF.
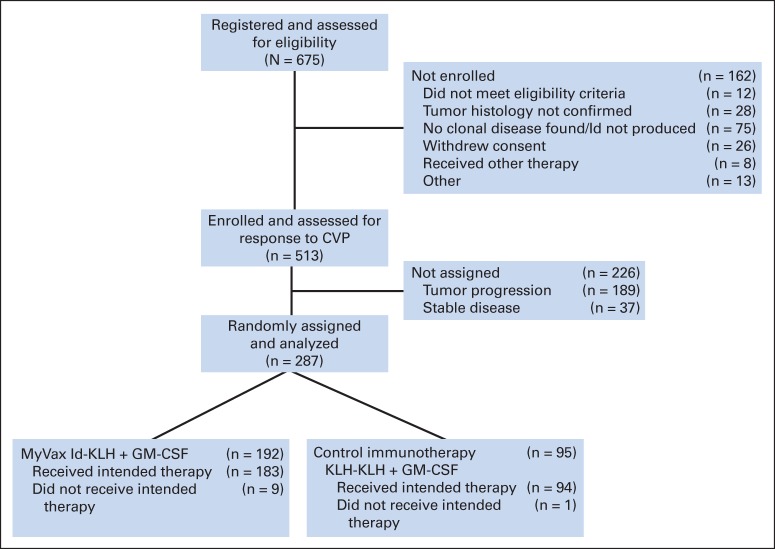
Patients and methods: Patients with previously untreated advanced-stage follicular lymphoma (FL) received eight cycles of chemotherapy with cyclophosphamide, vincristine, and prednisone. Those achieving sustained partial or complete remission (n=287 [44%]) were randomly assigned at a ratio of 2:1 to receive one injection per month for 7 months of MyVax or control immunotherapy. Anti-Id antibody responses (humoral immune responses [IRs]) were measured before each immunization. The primary end point was progression-free survival (PFS). Secondary end points included IR and time to subsequent antilymphoma therapy.
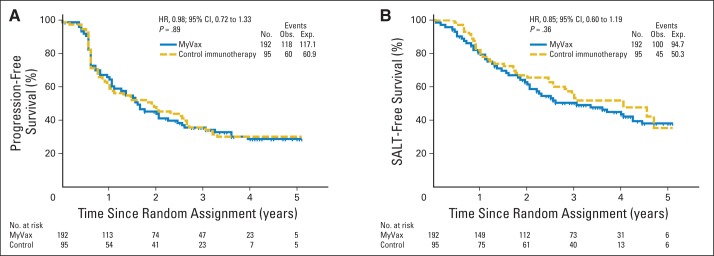
Results: At a median follow-up of 58 months, no significant difference was observed in either PFS or time to next therapy between the two arms. In the MyVax group (n=195), anti-Id IRs were observed in 41% of patients, with a median PFS of 40 months, significantly exceeding the median PFS observed in patients without such Id-induced IRs and in those receiving control immunotherapy.
Conclusion: This trial failed to demonstrate clinical benefit of specific immunotherapy. The subset of vaccinated patients mounting specific anti-Id responses had superior outcomes. Whether this reflects a therapeutic benefit or is a marker for more favorable underlying prognosis requires further study.
Trial registration: ClinicalTrials.gov NCT00017290.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

Comment in
-
Immune responses and outcome in follicular lymphoma.J Clin Oncol. 2014 Jun 10;32(17):1757-9. doi: 10.1200/JCO.2013.53.8439. Epub 2014 May 5. J Clin Oncol. 2014. PMID: 24799493 No abstract available.
References
-
- Hiddemann W, Kneba M, Dreyling M, et al. Frontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) significantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: Results of a prospective randomized study of the German Low-Grade Lymphoma Study Group. Blood. 2005;106:3725–3732. - PubMed
-
- Marcus R, Imrie K, Belch A, et al. CVP chemotherapy plus rituximab compared with CVP as first-line treatment for advanced follicular lymphoma. Blood. 2005;105:1417–1423. - PubMed
-
- Marcus R, Imrie K, Solal-Celigny P, et al. Phase III study of R-CVP compared with cyclophosphamide, vincristine, and prednisone alone in patients with previously untreated advanced follicular lymphoma. J Clin Oncol. 2008;26:4579–4586. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
