

Capecitabine and oxaliplatin in the preoperative multimodality treatment of rectal cancer: surgical end points from National Surgical Adjuvant Breast and Bowel Project trial R-04
- PMID: 24799484
- PMCID: PMC4050205
- DOI: 10.1200/JCO.2013.53.7753
Capecitabine and oxaliplatin in the preoperative multimodality treatment of rectal cancer: surgical end points from National Surgical Adjuvant Breast and Bowel Project trial R-04
Abstract
Purpose: The optimal chemotherapy regimen administered concurrently with preoperative radiation therapy (RT) for patients with rectal cancer is unknown. National Surgical Adjuvant Breast and Bowel Project trial R-04 compared four chemotherapy regimens administered concomitantly with RT.
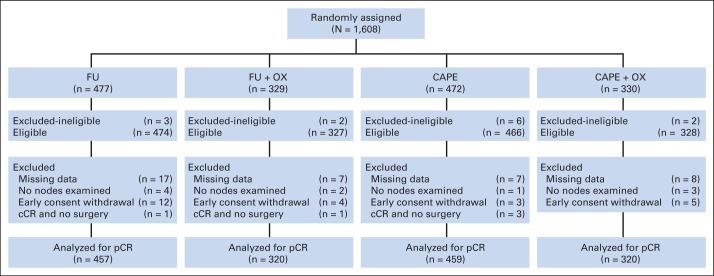
Patients and methods: Patients with clinical stage II or III rectal cancer who were undergoing preoperative RT (45 Gy in 25 fractions over 5 weeks plus a boost of 5.4 Gy to 10.8 Gy in three to six daily fractions) were randomly assigned to one of the following chemotherapy regimens: continuous intravenous infusional fluorouracil (CVI FU; 225 mg/m(2), 5 days per week), with or without intravenous oxaliplatin (50 mg/m(2) once per week for 5 weeks) or oral capecitabine (825 mg/m(2) twice per day, 5 days per week), with or without oxaliplatin (50 mg/m(2) once per week for 5 weeks). Before random assignment, the surgeon indicated whether the patient was eligible for sphincter-sparing surgery based on clinical staging. The surgical end points were complete pathologic response (pCR), sphincter-sparing surgery, and surgical downstaging (conversion to sphincter-sparing surgery).
Results: From September 2004 to August 2010, 1,608 patients were randomly assigned. No significant differences in the rates of pCR, sphincter-sparing surgery, or surgical downstaging were identified between the CVI FU and capecitabine regimens or between the two regimens with or without oxaliplatin. Patients treated with oxaliplatin experienced significantly more grade 3 or 4 diarrhea (P < .001).
Conclusion: Administering capecitabine with preoperative RT achieved similar rates of pCR, sphincter-sparing surgery, and surgical downstaging compared with CVI FU. Adding oxaliplatin did not improve surgical outcomes but added significant toxicity. The definitive analysis of local tumor control, disease-free survival, and overall survival will be performed when the protocol-specified number of events has occurred.
Trial registration: ClinicalTrials.gov NCT00058474.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Gunderson LL, Sargent DJ, Tepper JE, et al. Impact of T and N stage and treatment on survival and relapse in adjuvant rectal cancer: A pooled analysis. J Clin Oncol. 2004;22:1785–1796. - PubMed
-
- Gastrointestinal Tumor Study Group. Prolongation of the disease-free interval in surgically treated rectal carcinoma: Gastrointestinal Tumor Study Group. N Engl J Med. 1985;312:1465–1472. - PubMed
-
- Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med. 1991;324:709–715. - PubMed
-
- Wolmark N, Wieand HS, Hyams DM, et al. Randomized trial of postoperative adjuvant chemotherapy with or without radiotherapy for carcinoma of the rectum: National Surgical Adjuvant Breast and Bowel Project Protocol R-02. J Natl Cancer Inst. 2000;92:388–396. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10-CA-37377/CA/NCI NIH HHS/United States
- N01 CA032102/CA/NCI NIH HHS/United States
- U10 CA012027/CA/NCI NIH HHS/United States
- U-10-CA-69974/CA/NCI NIH HHS/United States
- U10-CA-12027/CA/NCI NIH HHS/United States
- CA22453/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- P30 CA022453/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180868/CA/NCI NIH HHS/United States
- U10-CA-69651/CA/NCI NIH HHS/United States
- U10 CA069651/CA/NCI NIH HHS/United States
- U10 CA032102/CA/NCI NIH HHS/United States
- U10 CA069974/CA/NCI NIH HHS/United States
- CA032102/CA/NCI NIH HHS/United States
- U10 CA037377/CA/NCI NIH HHS/United States
- P30 CA056036/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
